
Osteomyelitis (plural: osteomyelitides) refers to infection, typically bacterial, of bone involving the medullary cavity 21.
This article is focused on acute bacterial osteomyelitis. Other types of osteomyelitis are discussed separately:
Bone infection is one of the "I"s in the popular mnemonic for lucent bone lesions FEGNOMASHIC.
On this page:
Diagnosis
The pathological diagnosis of osteomyelitis requires a reliable tissue sample from which bacteria are isolated, along with histological findings of inflammatory cells and osteonecrosis 21.
Given low culture yields (~35%), pathological testing often results in false-negative results. Osteomyelitis can be diagnosed on MRI in cases of suspected infection where there are concordant bone marrow signal changes of low T1 signal, high signal on fluid-weighted sequences, and post-contrast enhancement 21.
The phrase "high likelihood of osteomyelitis" is recommended where there is bone marrow high signal on fluid-weight sequences adjacent to an ulcer, abscess, or sinus tract, no matter the T1 signal intensity 21.
Terminology
Reactive bone marrow oedema and osteitis are recommended to be avoided in cases of infection as these can occur in non-infectious conditions, e.g. inflammatory arthritis 21.
Acute osteomyelitis is where symptoms are present for <2 weeks and chronic osteomyelitis is where symptoms are present for >4 weeks 21.
Epidemiology
Osteomyelitis can occur at any age. In those without specific risk factors, it is particularly common between the ages of 2-12 years and is more common in males (M:F of 3:1) 6.
Pathology
In most instances, osteomyelitis results from haematogenous spread, although direct extension from trauma and/or ulcers is relatively common (especially in the feet of diabetic patients).
In the initial stages of infection, bacteria multiply, triggering a localised inflammatory reaction that results in localised cell death. With time, the infection becomes demarcated by a rim of granulation tissue and new bone deposition.
Although no organisms are cultured from tissue sampling in ~35% (range 21-50%) of cases 1,21, when one is isolated, Staphylococcus aureus is by far the most common pathogen. Different organisms are more common in specific clinical scenarios 1,4,21:
Staphylococcus aureus: 80-90% of all infections; includes meticillin-resistant isolates (MRSA)
Escherichia coli: intravenous drug users (IVDU) and genitourinary tract infection
Pseudomonas spp.: intravenous drug use and genitourinary tract infection
Klebsiella spp.: intravenous drug use and genitourinary tract infection
Salmonella spp.: sickle cell disease
Haemophilus influenzae: neonates
group B streptococci: neonates
Other uncommon infective agents include fungi (see: fungal osteomyelitis).
Location
Frequency by location, in descending order 18:
lower limb (most common)
vertebrae: lumbar > thoracic > cervical
radial styloid
The location of osteomyelitis within a bone varies with age, on account of changes in vascularisation of different parts of the bone 1,4:
neonates: metaphysis and/or epiphysis
children: metaphysis
adults: epiphyses and subchondral regions
Variants
Radiographic features
MRI has the highest accuracy to detect osteomyelitis with a sensitivity of 90% and specificity of ~80% 21. In some instances, imaging features are specific to a region or a particular type of infection, for example:
Below are the general features of osteomyelitis.
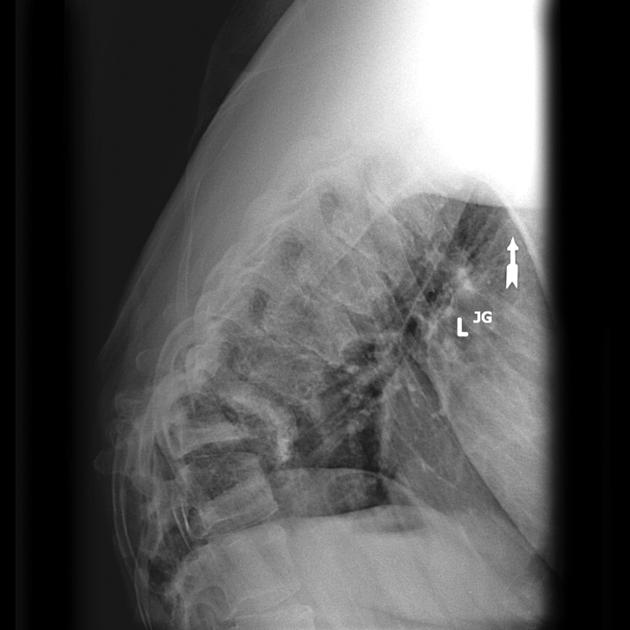
Plain radiograph
The earliest changes are seen in adjacent soft tissues +/- muscle outlines with swelling and loss or blurring of normal fat planes. An effusion may be seen in an adjacent joint.
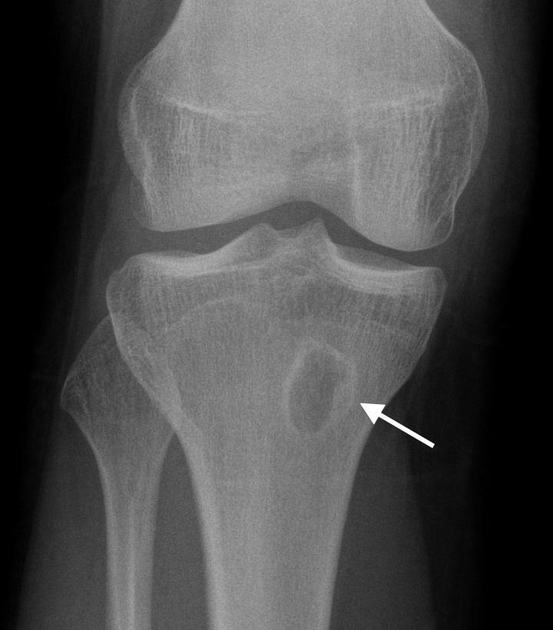
In general, osteomyelitis must extend at least 1 cm and compromise ~40% (range 30-50%) of bone mineral content to produce noticeable changes on plain radiographs ref. Early findings may be subtle, and changes may not be obvious until 5 to 7 days from the onset in children and 10 to 14 days in adults ref. On radiographs taken after this time period, a number of changes may be noted ref:
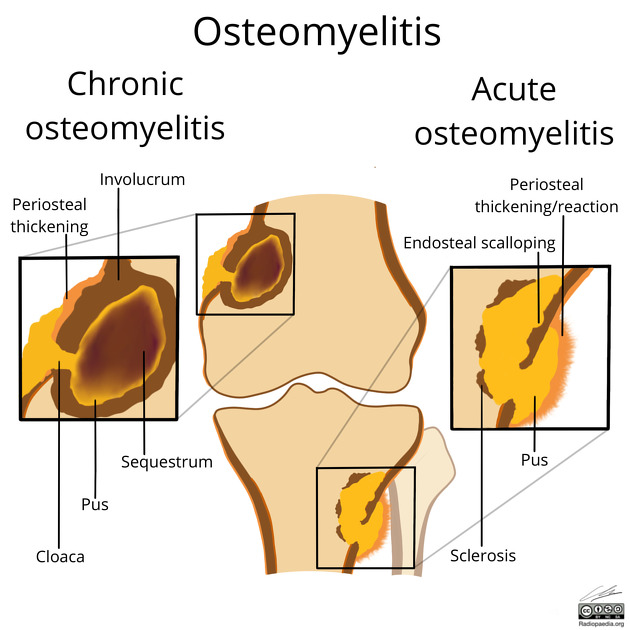
periosteal reaction/thickening (periostitis): variable; may appear aggressive, including the formation of a Codman's triangle 6
focal bony lysis or cortical loss
loss of trabecular bone architecture
new bone apposition
eventual peripheral sclerosis
In chronic or untreated cases, chronic osteomyelitis with distinctive imaging characteristics may develop.
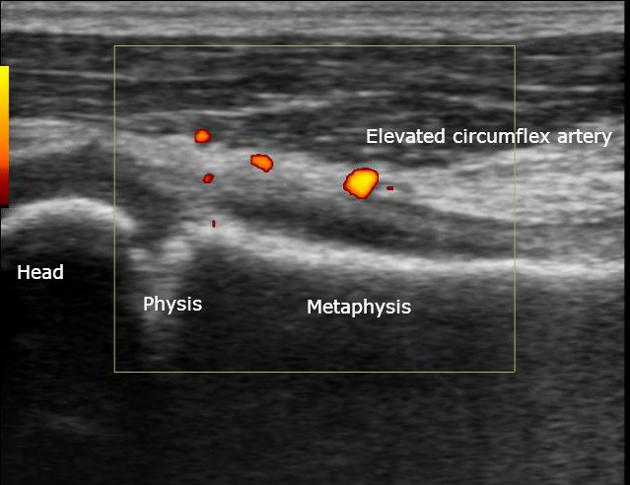
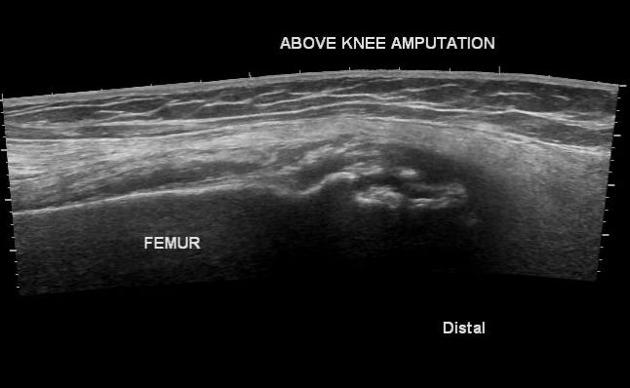
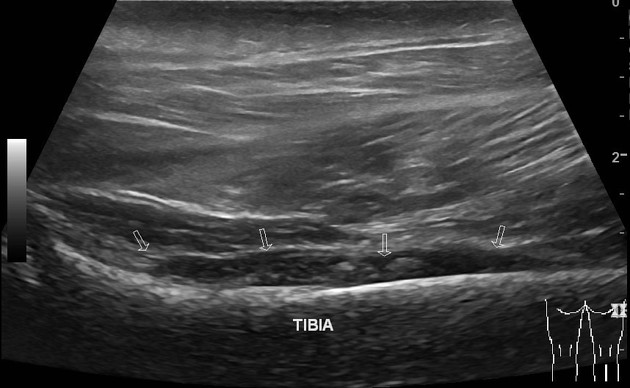
Ultrasound
Although ultrasound excels as a fast and inexpensive examination of the soft tissues and can guide the drainage of soft tissue collections, it has little role in the direct assessment of osteomyelitis, as it is unable to visualise within the bone ref.
It does, however, have a role in the assessment of soft tissues and joints adjacent to infected bone, as it can be used to visualise soft tissue abscesses, cellulitis, subperiosteal collections, and joint effusion ref.
Ultrasound is also useful in assessing the extraosseous components of orthopaedic instrumentation, as it is not affected by metal artifacts 3.
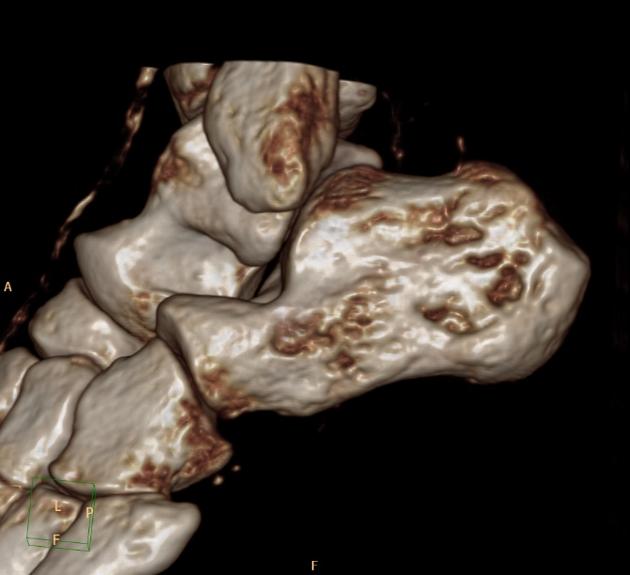
CT
CT is superior to both MRI and plain radiographs in depicting the bony margins and identifying a sequestrum or involucrum. The CT features are otherwise similar to plain radiographs. The overall sensitivity and specificity of CT is low, even in the setting of chronic osteomyelitis, and according to one study are 67% and 50%, respectively 17.
Intravenous contrast allows CT to differentiate between different tissue types and characterise abscesses 22, but is inferior to MRI scan in this aspect 24.
Some features on CT include 23:
blurring of fat planes
increased density of fatty marrow
periosteal reaction
cortical erosion/destruction
sequestra, involucra, intraosseus gases in chronic osteomyelitis
Some limitations CT include 20:
inability to confidently detect marrow oedema; therefore, a normal CT does not exclude early osteomyelitis.
image degradation by streak artifact when metallic implants are present
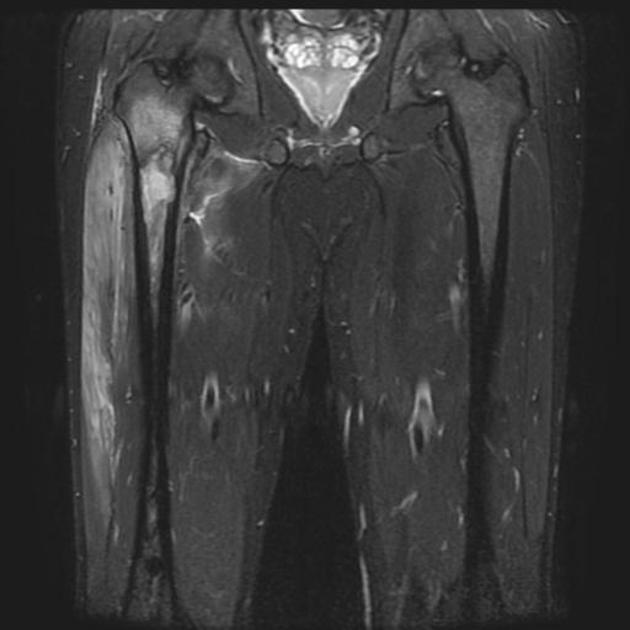
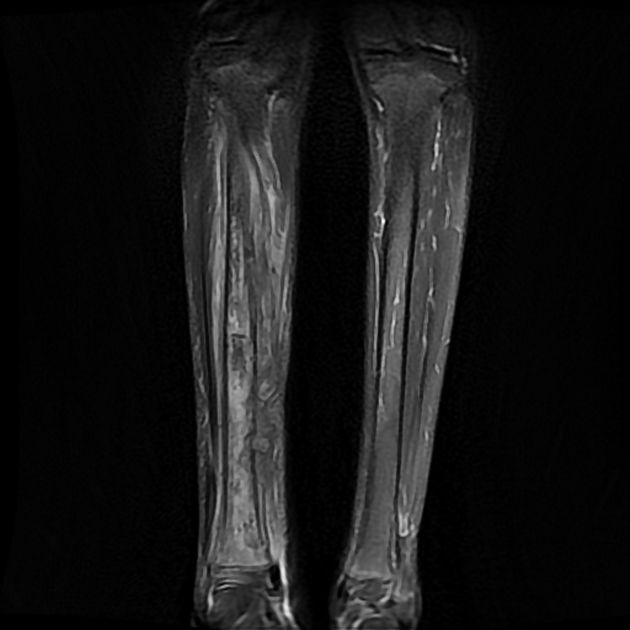
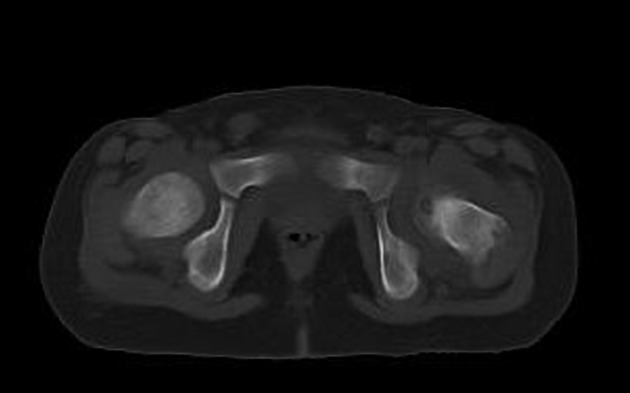
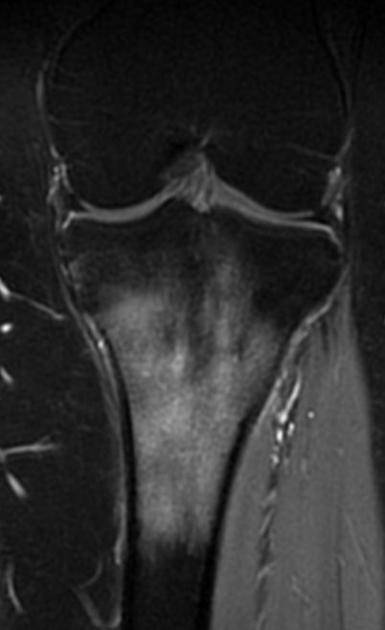
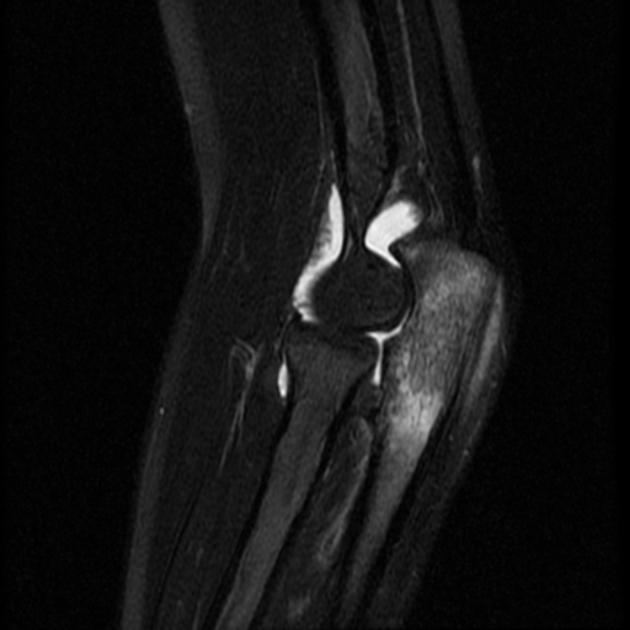
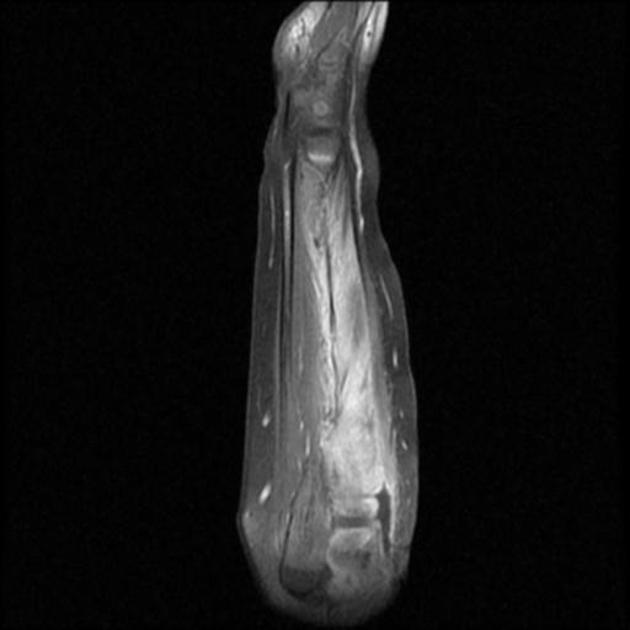
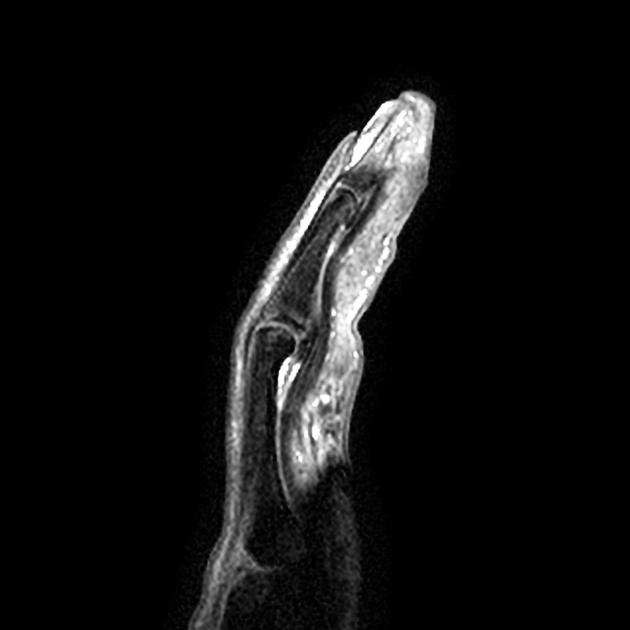
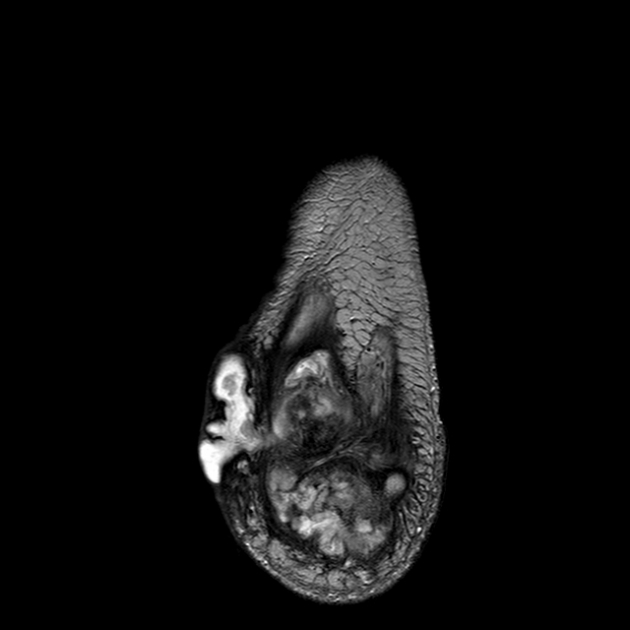
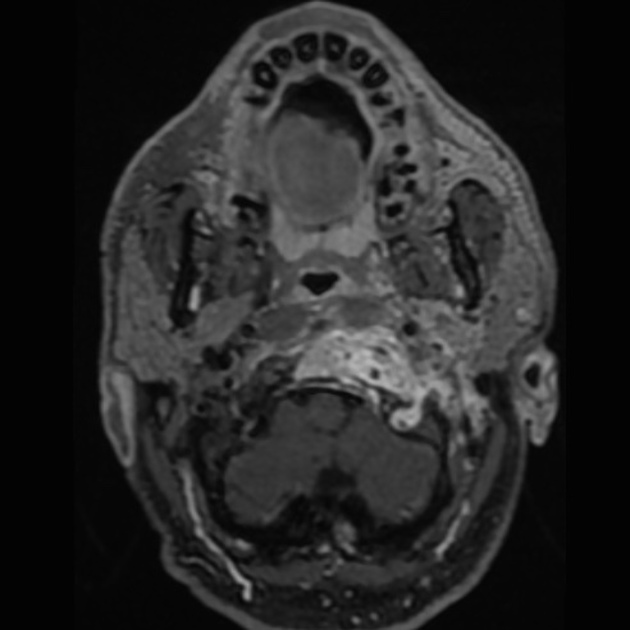
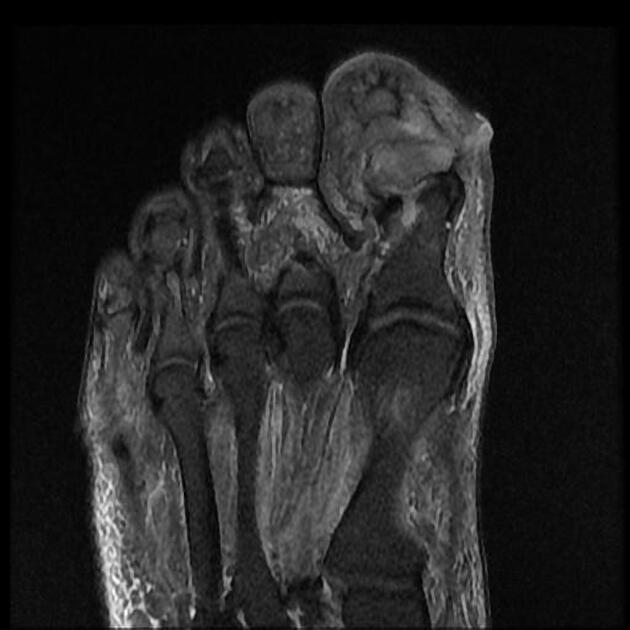
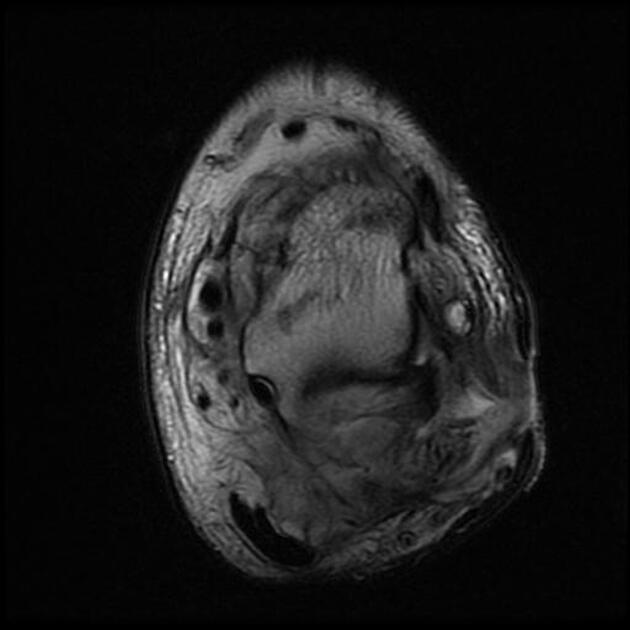
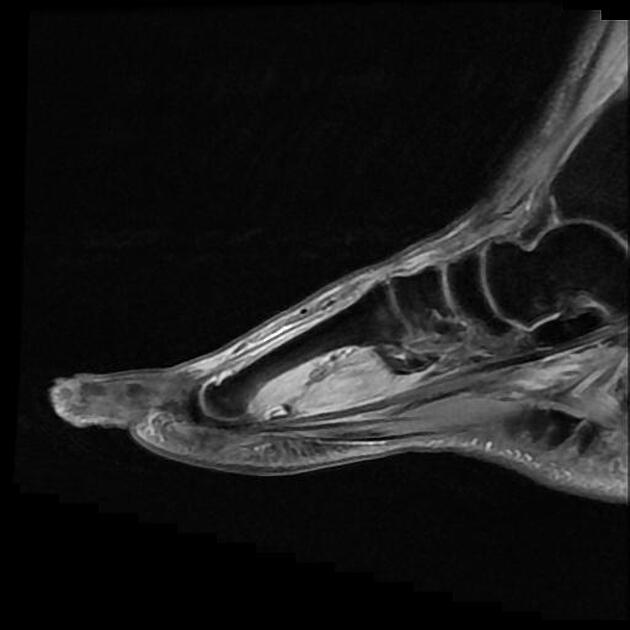
MRI
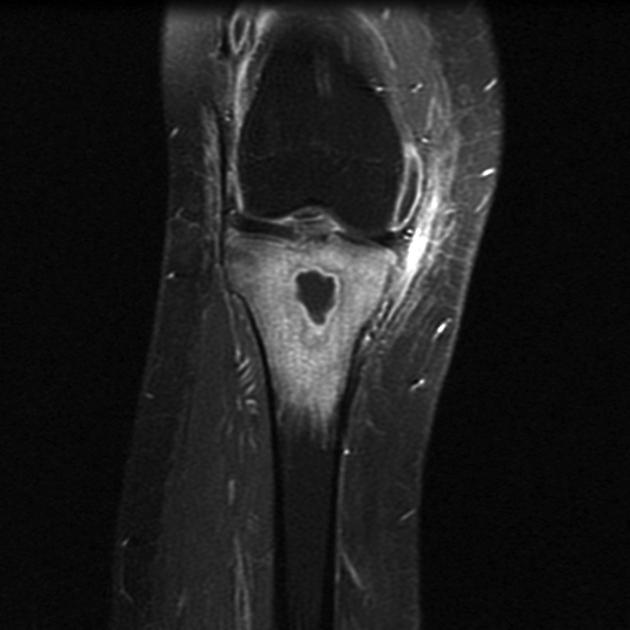
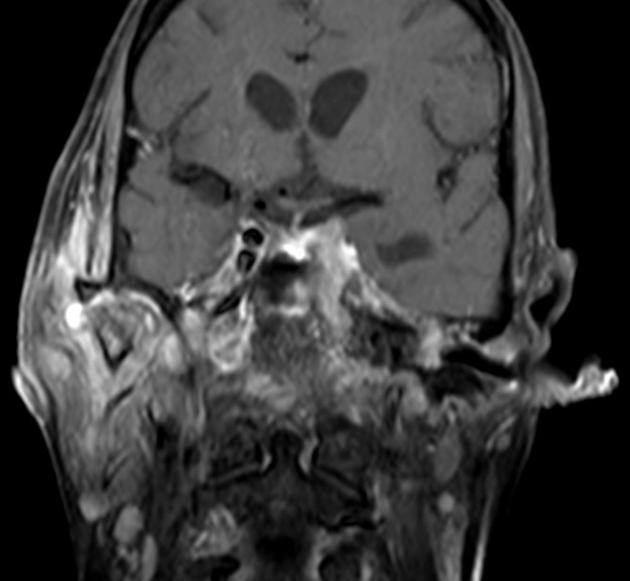
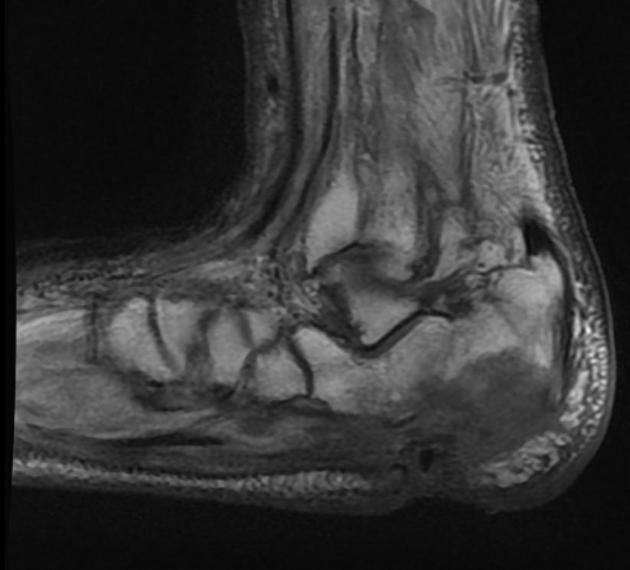
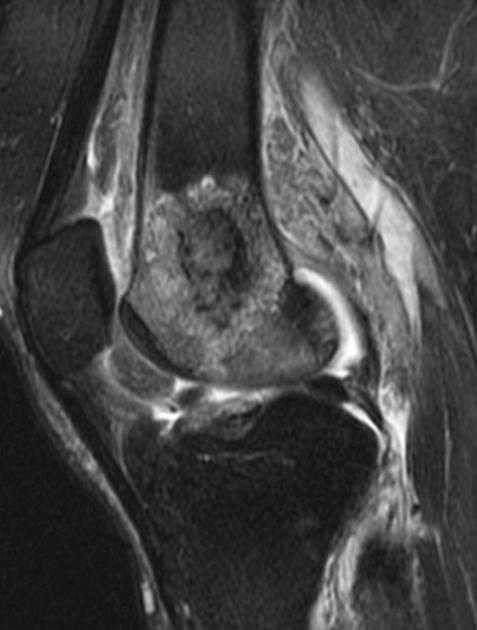
MRI is the most sensitive and specific and is able to identify soft-tissue/joint complications 5,14. Bone marrow oedema is the earliest feature of acute osteomyelitis seen on MRI and can be detected as early as 1 to 2 days after the onset of infection 20. Concordant low signal T1 and high signal on fluid-sensitive sequences is the hallmark of osteomyelitis on MRI 21.
-
T1
intermediate to low signal central component
surrounding bone marrow of lower signal than normal due to oedema
cortical bone destruction
-
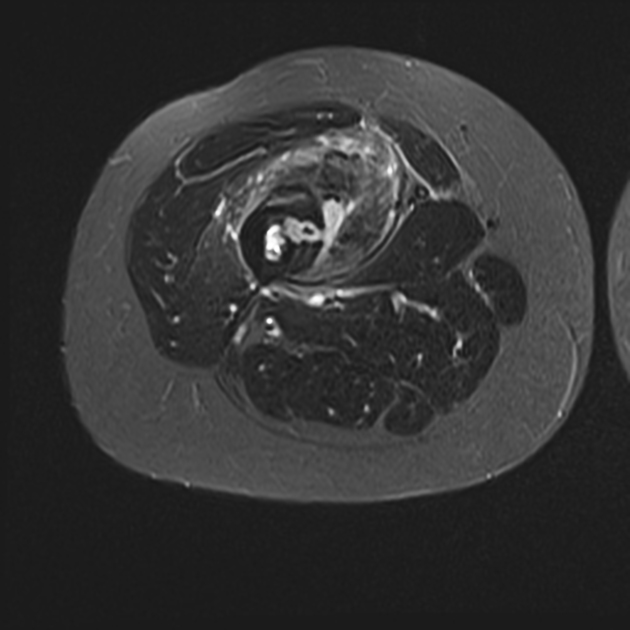
T2
bone marrow high signal
T1 C+ (Gd): post-contrast enhancement of bone marrow, abscess margins, periosteum, and adjacent soft tissue collections
Where there is discordant bone marrow signal change (i.e. high signal on fluid-sensitive sequences but normal T1 signal), the more intense the signal is on fluid-sensitive sequences is (i.e. similar to joint fluid signal), the more likely osteomyelitis is to be present or subsequently develop 21.
Nuclear medicine
A number of techniques may be employed to detect foci of osteomyelitis.
These include 2:
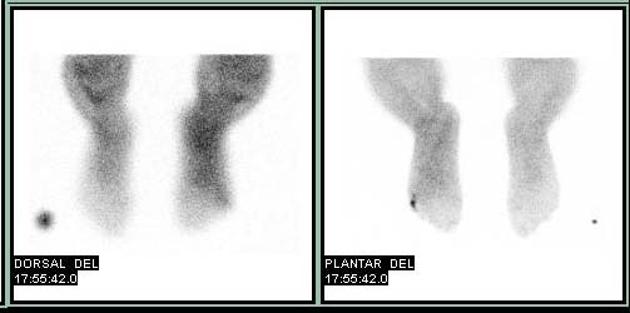
Bone scintigraphy (Tc-99m)
Increased osteoblastic activity results in increased levels of radiotracer uptake in the surrounding bone, usually both on blood pool and delayed views. It is highly sensitive but not particularly specific.
Indium-111 labelled WBC scintigraphy
It may be useful in cases of:
diabetic osteomyelitis, especially combined with Tc-99m-phosphonate imaging 2,7; however, MRI is now generally used in conjunction with plain films 14,15
orthopaedic implants
vertebral osteomyelitis (Ga-67 is best) 2
ulcers in bedridden patients with potential underlying osteomyelitis (In-111 with Tc-99m-phosphonate)
Gallium-67 scintigraphy
radiogallium attaches to transferrin, which leaks from the bloodstream into areas of inflammation, showing increased isotope uptake in infection, sterile inflammatory conditions, and malignancy
imaging is usually performed 18 to 72 hours after injection and is often performed in conjunction with radionuclide bone imaging
one difficulty with gallium is that it does not show bone detail particularly well and may not distinguish well between bone and nearby soft tissue inflammation
gallium scans may reveal abnormal accumulation in patients who have active osteomyelitis when technetium scans reveal decreased activity (“cold” lesions) or perhaps normal activity
gallium accumulation may correlate more closely with inflammatory activity in cases of osteomyelitis than does technetium uptake
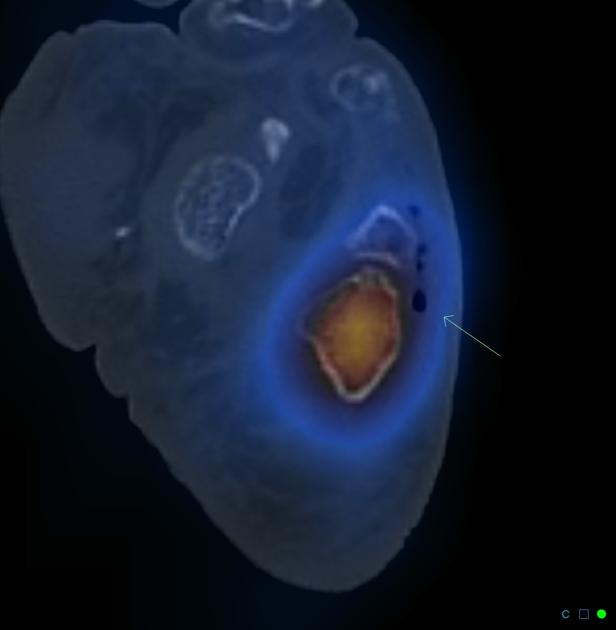
PET-CT
PET-CT systems are relatively novel techniques that are being applied. FDG-PET may have the highest diagnostic accuracy for confirming or excluding chronic osteomyelitis in comparison with bone scintigraphy, MRI, or leucocyte scintigraphy. It is also considered superior to leucocyte scintigraphy in detecting chronic osteomyelitis in the axial skeleton 9.
Treatment and prognosis
Treatment of osteomyelitis is typical with intravenous antibiotics, often for extended periods. If a collection, sequestrum, or involucrum is present, drainage and/or surgical debridement is often necessary. Amputation is performed after failure of medical therapy or when the infection is life-threatening.
Complications include 1:
sinus tract formation with occasional superimposed squamous cell carcinoma (Marjolin ulcer)
secondary sarcoma (e.g. osteosarcoma): rare
Differential diagnosis
General imaging differential considerations include:
-
primary bone neoplasm





























 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.