
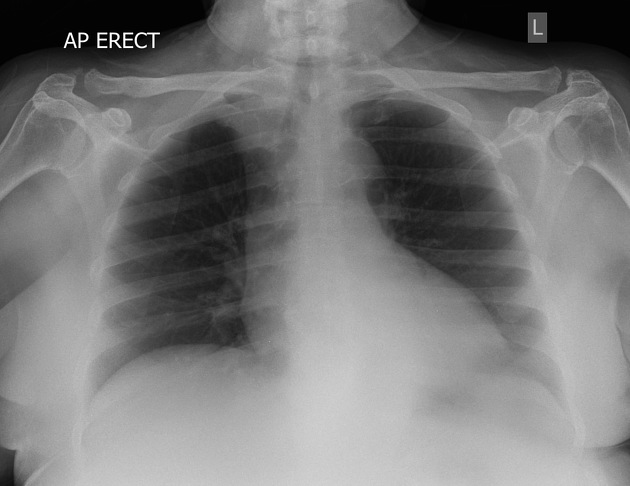
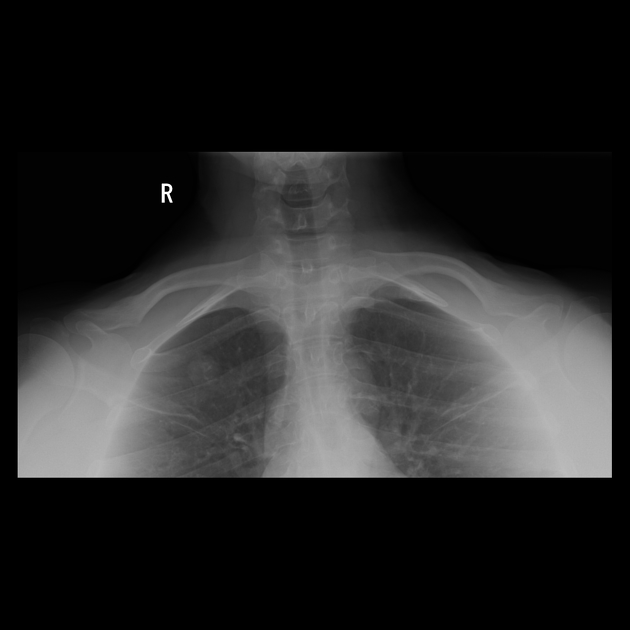
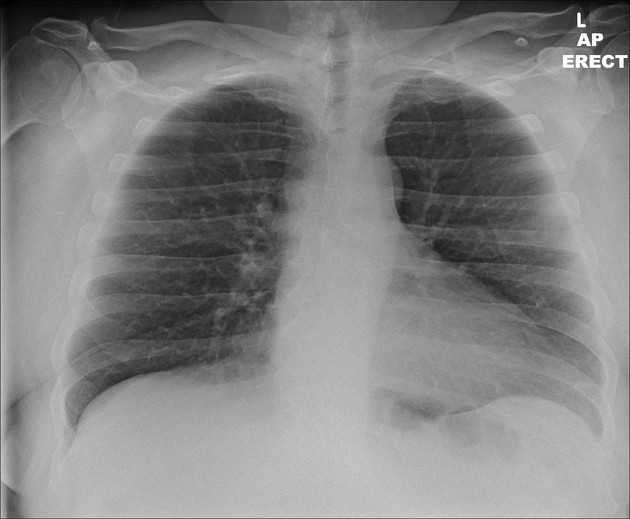
The AP lordotic chest radiograph (or AP axial chest radiograph) demonstrates areas of the lung apices that appear obscured on the PA/AP chest radiographic views.
On this page:
Indication
The AP lordotic projection is often used to evaluate suspicious areas within the lung apices that appeared obscured by overlying soft tissue, upper ribs or the clavicles on previous chest views (e.g. in cases of tuberculosis or tumor).
Patient position
the patient is standing with feet approximately 30 cm away from the image receptor, with back arched until upper back, shoulders and head are against the image receptor
the shoulders and elbows are rolled anteriorly
the angle formed between the midcoronal body plane and image receptor should be approximately 45 degrees
Technical factors
anteroposterior projection
suspended inspiration
-
centering point
midsagittal plane, halfway between the manubriosternal junction and the xiphoid process
-
collimation
superiorly 5 cm above the shoulder joint to allow proper visualization of the upper airways
inferior to the inferior border of the 12th rib
lateral to the level of the acromioclavicular joints
-
orientation
portrait or landscape
-
detector size
35 cm x 43 cm or 43 cm x 35 cm
-
exposure
100-110 kVp
4-8 mAs
-
SID
180 cm
-
grid
yes (this may be departmentally dependent)
Image technical evaluation
superior lung fields should be in the middle of the image with the clavicles, lung apices and two thirds of the lungs within the collimation field
sternoclavicular ends of the clavicles should be projected above the lung apices, and the first to fourth ribs should appear horizontal and near superimposed, demonstrating a correct lordotic position and/or angle
lateral borders of the scapulae demonstrated away from the lung fields, demonstrating sufficient anterior rotation of the patient’s shoulders and elbows
there should be equal distances from the vertebral column to the sternal clavicular ends, demonstrating no rotation
the clavicles should appear in the same horizontal plane, and projected above lung apices
Practical points
there are several ways to accomplish this view, should the patient be unable to achieve the aforementioned positioning; the patient can remain completely upright with upper back and shoulders against the image receptor and a 45-degree cephalic central ray angulation used to project the clavicles above the apices; this positioning option can be used to achieve this radiographic view with a supine patient
a combination of positions can also be utilized, with the patient’s back arched as much as possible and the central ray angled cephalically the amount necessary to equal a 45-degree angle
patients with a long-standing history of emphysema or COPD will have abnormally long lungs compared to the general population, remember this when collimating superior to inferior
side marker placement is imperative; patients can have congenital conditions that mimic a mirrored image 2
remember to explain to your patient what you are about to do; remember to ask them to take a breath in and hold it; many times this gives the patient time to prepare and results in a better breath hold and therefore a higher quality radiograph
same positioning but different collimation is used to better visualization of middle lobe and lingual lobe pathologies as they get the maximum thickness for X-ray beam to pass in this positioning
History and etymology
It is said that Felix Fleischner (1893-1969) first advocated the lordotic projection, in an article published in 1926. However, it was likely used before that time 3,4.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.