
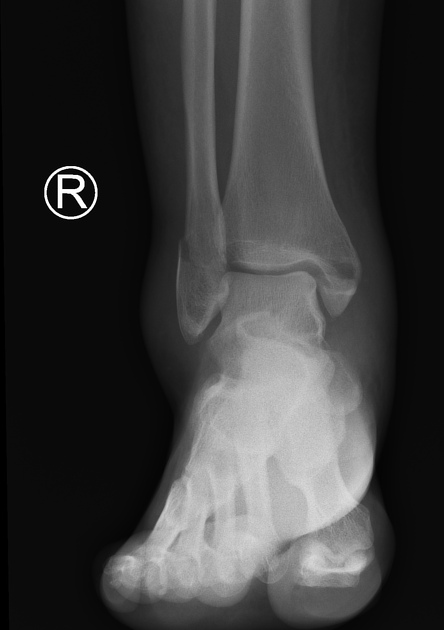
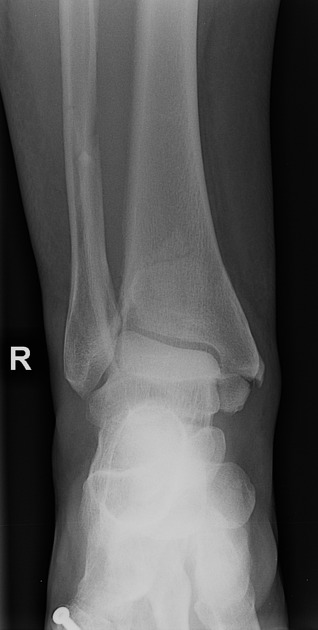
The ankle AP view is part of a three view series, and visualizes the distal tibia, distal fibula, proximal talus and proximal fifth metatarsal.
On this page:
Indications
The true anteroposterior view of the ankle is often performed in the setting of ankle trauma and suspected ankle fractures in addition to the lateral and mortise views of the ankle.
Other indications include:
assessment of fragment position and implants in postoperative follow up
evaluation of fracture healing
evaluation of tibiofibular clear space and overlap in suspected syndesmotic injury
evaluation of hindfoot deformities
In addition, this view can show bony diseases or lesions of the distal lower leg, talus and proximal fifth metatarsal.
Patient position
the patient may be supine or sitting upright with their leg straighten on the table
the foot is in dorsiflexion
the toes will be pointing directly toward the ceiling
Technical factors
anteroposterior projection
-
centering point
the midpoint of the lateral and medial malleoli
-
collimation
laterally to the skin margins
superior to examine the distal third of the tibia and fibula
inferior to the proximal aspect of the metatarsals
-
orientation
portrait
-
detector size
24 cm x 30 cm
-
exposure
50-60 kVp
3-5 mAs
-
SID
100 cm
-
grid
no
Image technical evaluation
the distal fibula should be slightly superimposed the distal tibia
the lateral and medial malleoli of the distal fibula and tibia are in profile
the tibiotalar joint space should be open, yet the full mortise joint should not be visualized on the AP
Practical points
This view can be thought of as the literal anteroposterior of the ankle. Most patients will naturally place their foot in this position.
Although dorsiflexion is essential in both the AP and the mortise view it should be noted that during trauma this may not be possible.







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.