
The coccyx (plural: coccyges) is the series of rudimentary vertebrae forming the caudal termination of the vertebral column and is positioned inferior to the apex of the sacrum. The coccyx is one leg of the tripod formed in conjunction with the ischial tuberosities for support in a seated position. Additionally, it serves as the insertion site for the muscles of the pelvic floor and those that contribute to voluntary bowel control and supports the position of the anus.
On this page:
Terminology
For the purposes of numbering the vertebral segments, and stipulated by the Terminologia Anatomica (TA), "Co" is used as the abbreviation for each coccygeal level, e.g. Co1, Co2, etc. Clearly "C" is already used for the cervical vertebrae.
Gross anatomy
The coccyx is formed from four rudimentary vertebrae and does not contain a spinal canal, pedicles, laminae or spinous processes. The first segment is the largest, and the subsequent are smaller in size. Structure of the coccygeal vertebral junctions is variable and age-related, ranging from fully developed to rudimentary intervertebral discs with varying degrees of cystic or fibrotic change, to fusion of the vertebrae in the later decades.
The coccyx consists of an anterior and posterior surface, two lateral surfaces, an apex and a base.
anterior surface: concave, marked with three transverse grooves representing the fusions of the four separate vertebrae
-
posterior surface
convex, similarly marked with three transverse grooves
there is a vertical row of tubercles on either side, which are rudimentary articular processes of the coccygeal vertebrae
the superior pair are the largest and are called the coccygeal cornua. They articulate with the sacral cornua
the coccygeal and sacral cornua combine to form the foramen for the transmission of the posterior division of the fifth sacral nerve
-
lateral surface
thin with several eminences that represent rudimentary transverse processes of the coccygeal vertebrae
the most superior eminences join the lateral edges of the sacrum, forming the foramen for the transmission of the anterior division of the fifth sacral nerve
it is the largest eminence and the inferior eminences subsequently decrease in size
anteriorly to posteriorly, the lateral border serves as attachment for the coccygeus, sacrospinous ligament, sacrotuberous ligament, and fibers of the gluteus maximus
base: proximal oval surface for articulation with the sacrum
apex: distal rounded prominence
Articulations
-
sacrococcygeal symphysis
fibrocartilaginous joint that connects the apex of the sacrum to the coccyx
movement is passive minor flexion and extension
typically fuses with age
Attachments
Ligamentous
Five ligaments support the sacrococcygeal symphysis:
anterior sacrococcygeal ligament: continuation of the anterior longitudinal ligament - connects to the anterior aspect of the 1st and sometimes 2nd vertebral bodies
deep posterior sacrococcygeal ligament: connects from the 5th sacral body to the dorsal surface of the coccyx
superficial posterior sacrococcygeal ligament: begins on the medial sacral crest and inserts on the dorsal surface of the coccyx
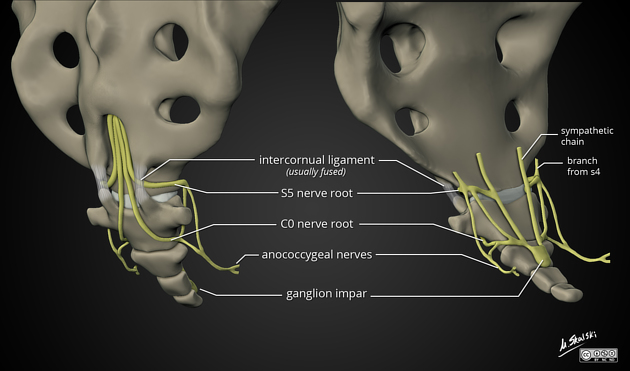
lateral sacrococcygeal ligament: joins the transverse process of the first coccygeal vertebra to the inferolateral angle of the sacrum. This completes the foramen for the fifth sacral nerve anteriorly. Posteriorly the foramen is closed by the sacral and coccygeal cornua connected by the intercornual ligament
interarticular (intercornual) ligaments: connect the cornua of the sacrum to the cornua of the coccyx
anococcygeal raphe: ligament that helps support the position of the anus
Musculotendinous
gluteus maximus muscle: attaches to the lateral coccyx
levator ani muscle: attaches to the anterior border and the apex of the coccyx
sphincter ani externus: attaches to the apex of the coccyx
Relations
upper surface: pelvic floor, ganglion impar
lower surface: buttocks
Variant anatomy
incomplete fusion
Variation in position
One method of classification on that was proposed by Postacchini and Massobrio and subsequently modified by Nathan which classifies into 6 types 8
type I: present in over half of people; coccyx has a gentle ventral curvature as a continuation of the natural curvature of the sacrum and a caudally pointing apex
type II: (8-32%): more prominent ventral curvature with coccyx apex pointing anteriorly
type III: (4-16%): acute anterior angulation of the coccyx but no subluxation
type IV: (1-9%): focal anterior angulation with anterior subluxation
type V: (1-11%): posteriorly angulated coccyx
type VI: (1-6%): scoliotic deformity or lateral deviation of coccyx
Radiographic features
Plain radiograph
AP axial and lateral views are used to visualize fractures.
Development
The coccyx arises from a caudal eminence present from weeks 4-8 of gestation. This caudal eminence regresses by birth, leaving the four precursor vertebrae. Each coccygeal segment is ossified from one primary center, with the cornua of the first segment ossifying from seperate centers 1. The first segment appears between ages one to four years, the second between ages five to ten years, the third between ten and fifteen years, and the fourth between fourteen and twenty years. Segments do not unite until after age twenty-five or thirty. The coccyx only fuses with the sacrum late in life, and this is more common in females than in males.
History and etymology
The word coccyx is derived from the Greek word for “cuckoo” because of its similarity to a cuckoo's beak when viewed from the side.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.