
Esophageal duplication cysts are congenital foregut duplication cysts.
On this page:
Epidemiology
Uncommon with a prevalence of 0.122% 9. There may be an increased male predilection 5.
Clinical presentation
Esophageal duplication cysts typically present in childhood with symptoms of dysphagia, cough, stridor, pain or arrhythmias 4. They can occur anywhere along the esophagus and about 90% have no communication with the oesopageal lumen. More than half occur in the lower third of the esophagus 4.
Pathology
They are a congenital malformation of the posterior primitive foregut and result from an aberration of the posterior division of the embryonic foregut at 3-4 weeks gestation. They are usually unilocular and contain mucin. The wall contains one or two smooth muscle layers and the inner epithelial lining is variable and can include stratified squamous, simple columnar, pseudostratified columnar, cuboidal, and ciliated epithelium. Islands of heterotopic gastric or pancreatic mucosa can cause ulceration, hemorrhage and perforation. The cyst may contain mucin and detached ciliary tufts.
Associations
Radiographic features
Plain radiograph
Well-defined soft tissue density in close association with the esophagus.
Fluoroscopy
On barium swallow, the cyst may cause extrinsic compression of the esophagus.
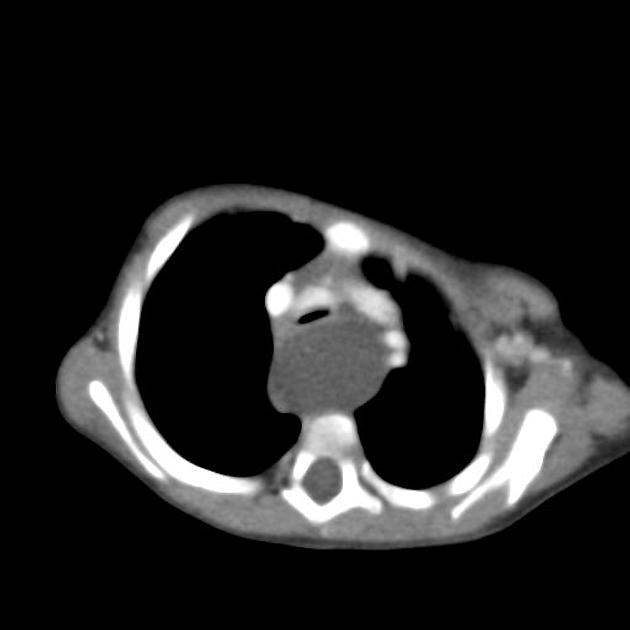
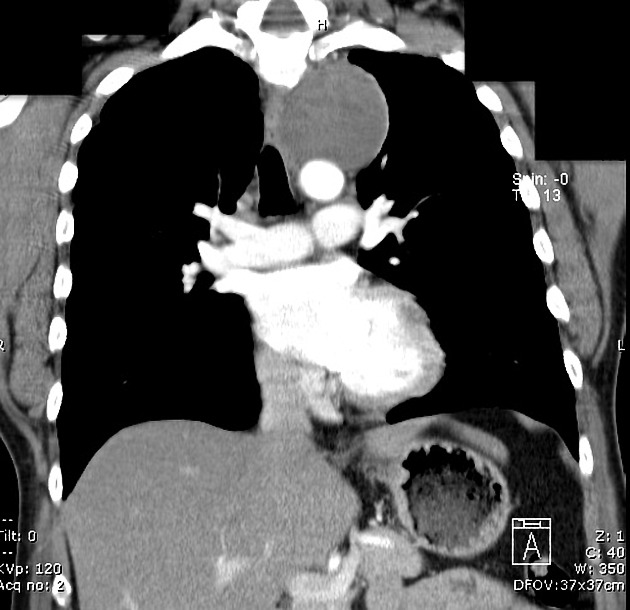
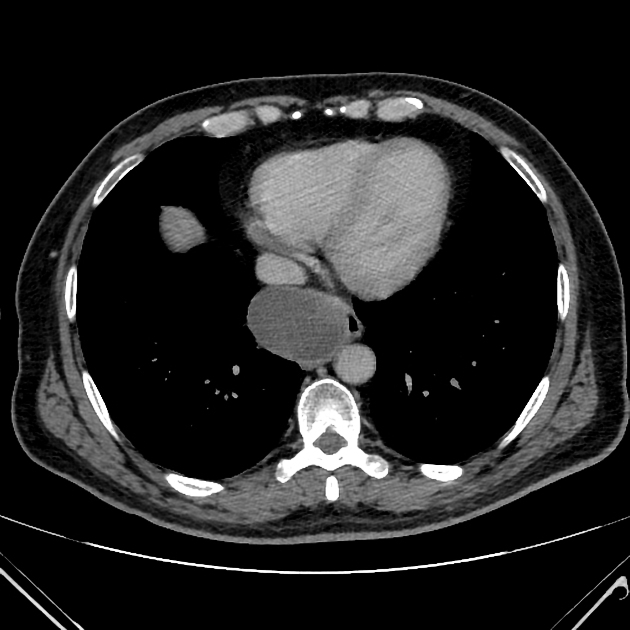
CT
Well-defined structure with internal fluid density along the esophagus. Its wall may be thicker than that of a bronchogenic cyst.
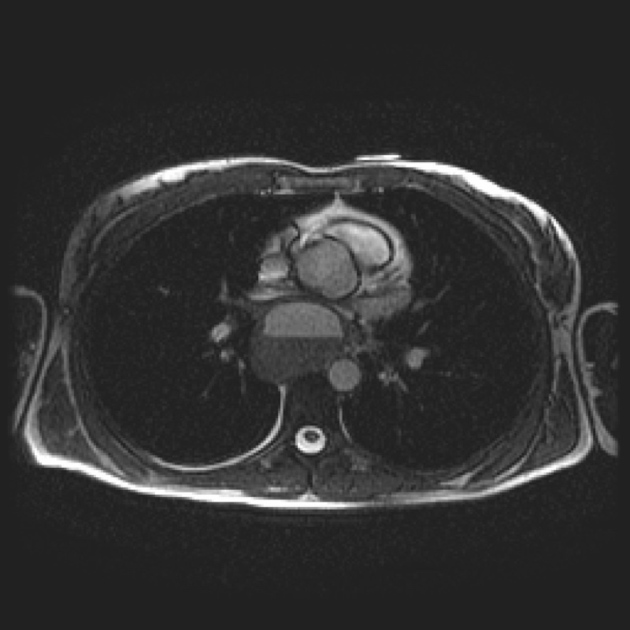
MRI
T1: low to intermediate signal intensity
T2: high signal intensity
Treatment and prognosis
Surgical resection is the mainstay of management for symptomatic cysts 8. Prognosis tends to be very good as recurrence is rare 8.
Complications
Recognized complications rarely include carcinoma arising within the cyst 5. If gastric mucosa is present peptic ulceration may occur. Very occasionally they may perforate, hemorrhage or erode into adjacent structures.
Biopsy is normally avoided due to the risk of infection and mediastinitis.
Differential diagnosis
For uncomplicated cysts consider:
-
congenital cysts and malformations in the region
cervical lymphadenopathy
pancreatic pseudocyst: for retroperitoneal bronchogenic cysts or for pancreatic pseudocysts that extend intrathoracically through the aortic or esophageal hiatus
For complicated cysts (e.g. with hemorrhage/necrosis), the differential can be broader and can include:
abscess(es)
enlarged lymph nodes (especially centrally necrotic)
-
pulmonary masses
hematoma




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.