
Radiographic evaluation of anterior cruciate ligament (ACL) reconstruction involves:
-
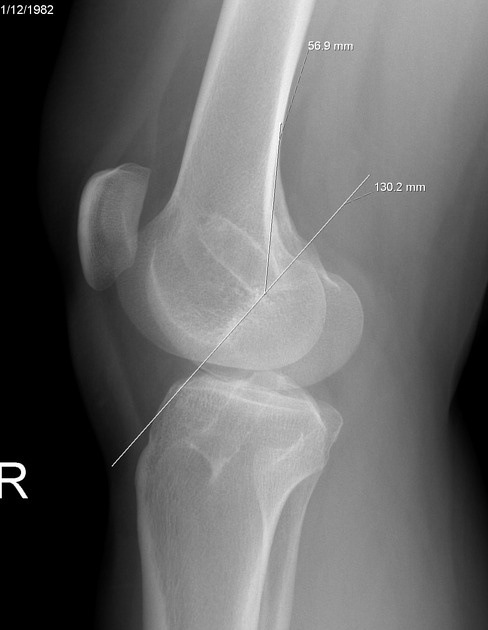
femoral component
a line is drawn along the posterior cortex of the femur
a second line is drawn along the roof of the intercondylar notch of the femur (Blumensaat line)
the point of intersection of these two lines should be at the inferior portion of the femoral component of the graft
the angle measured between a line drawn along the femur diaphysis and the femoral tunnel angle must be ~39°; angles of approximately ≤17° are associated with rotational instability
-
tibial component
The anterior wall of tibial tunnel should be entirely posterior to and parallel to the line drawn along the roof of the intercondylar notch (Blumensaat line). If the tibial component is too anterior the graft impingement or graft failure will happen, and if it is too posterior (vertical graft) the patient will suffer from a translational laxity.
when the femoral tunnel is drilled through the tibial tunnel, it is recommended to drill the tibial tunnel at an angle of 65° to 70° in the coronal plane, tibial tunnel angle of ≥72° is associated with greater loss of flexion and anterior laxity
-
tibial or femoral canal widening
loss of parallel walls and increase in diameter >2 mm from reconstruction time
-
hardware complications
migration of Endobutton into the femoral canal
interposing soft tissue between Endobutton and femoral shaft
migrated/displaced interference screw from the tibial or femoral canal
proud/intramuscular screw tip







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.