
ACR TI-RADS is a reporting system for thyroid nodules on ultrasound proposed by the American College of Radiology (ACR) 1.
This uses a standardized scoring system for reports providing users with recommendations for when to use fine needle aspiration (FNA) or ultrasound follow-up of suspicious nodules, and when to safely leave alone nodules that are benign/not suspicious.
On this page:
Radiographic features
Ultrasound
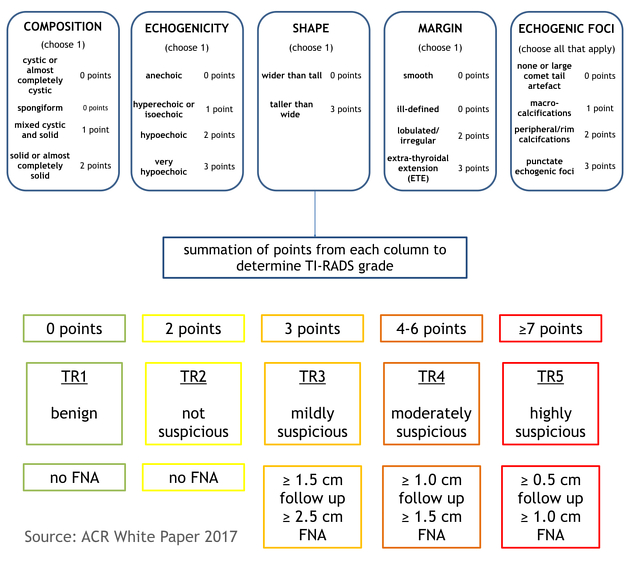
Scoring is determined from five categories of ultrasound findings (figure 2). The higher the cumulative score, the higher the TR (TI-RADS) level and the likelihood of malignancy.
One score is assigned from each of the following categories:
-
composition: (choose one)
cystic or completely cystic *: 0 points
spongiform *: 0 points
mixed cystic and solid: 1 point
solid or almost completely solid: 2 points
-
echogenicity: (choose one)
anechoic: 0 points
hyper- or isoechoic: 1 point
hypoechoic: 2 points
very hypoechoic: 3 points
-
shape: (choose one) (assessed on the transverse plane)
wider than tall: 0 points
taller than wide: 3 points
-
margin: (choose one)
smooth: 0 points
ill-defined: 0 points
lobulated/irregular: 2 points
extra-thyroidal extension: 3 points
Any and all findings in the final category are also added to the other four scores.
-
echogenic foci: (choose one or more)
none: 0 points
large comet-tail artifact: 0 points
macrocalcifications: 1 point
peripheral/rim calcifications: 2 points
punctate echogenic foci: 3 points
The findings in each category were detailed in the ACR committee's 2015 publication on a reporting lexicon 2. If multiple nodules are present only the four highest-scoring nodules (not necessarily the largest) should be scored, reported, and followed up.
* Predominantly cystic or spongiform nodules are inherently benign. If these features are present no further points will be added (automatically TR1).
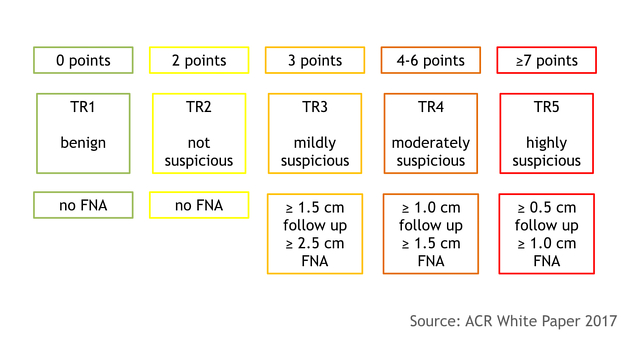
Scoring and classification
-
TR1: 0 points
benign
-
TR2: 2 points
not suspicious
-
TR3: 3 points
mildly suspicious
-
TR4: 4-6 points
moderately suspicious
-
TR5: ≥7 points
highly suspicious
Recommendations
TR1: no FNA required
TR2: no FNA required
-
TR3: ≥1.5 cm follow up, ≥2.5 cm FNA
follow up: 1, 3 and 5 years
-
TR4: ≥1.0 cm follow up, ≥1.5 cm FNA
follow up: 1, 2, 3 and 5 years
-
TR5: ≥0.5 cm follow up, ≥1.0 cm FNA
annual follow up for up to 5 years
FNA biopsy is recommended for suspicious lesions (TR3-TR5) with the above size criteria. If there are multiple nodules, the two with the highest ACR TI-RADS scores should be sampled (rather than the two largest), with largest size being used a tie-breaker if there are multiple nodules of the same classification.
Interval enlargement on follow-up is significant if there is an increase of >20% and >2 mm in two dimensions or a >50% increase in volume. If the ACR TI-RADS level increases between scans, an interval scan the following year is again recommended.
Risk of malignancy
The projected risk of malignancy in the original 2017 paper 1 was based on partial analysis of 3433 nodules with cytological results. Partial analysis at the time of publication showed rates of <2% for TR1/TR2, 5% for TR3, 5-20% for TR4 and >20% for TR5 nodules. The final analysis 4 demonstrated a stepwise increase for each point awarded by ACR TI-RADS, with each category validated. The published malignancy rates are:
TR1: 0.3%
TR2: 1.5%
TR3: 4.8%
TR4: 9.1%
TR5: 35%
Developments leading to ACR TI-RADS 2017
The previous ACR white paper from 2015 2 developed a lexicon from descriptive reports and this has been updated by the stratified scoring system in the 2017 white paper, rather than relying on a pattern-based system. Outcomes and recommendations are supported by another ACR paper on incidental thyroid nodules 3 and data from the Surveillance, Epidemiology, and End Results (SEER) programme of the National Cancer Institute.
The 2015 reporting lexicon 2 included 6 stages with a number of subdivisions (not replicated in this ACR TI-RADS) with increasing risk of malignancy.
The ACR system does not provide a grade for "normal thyroid gland" unlike other thyroid reporting systems, preserving ACR TI-RADS for lesion reporting. TR1 instead includes benign simple and/or spongiform cysts, each meeting 0 points from the criteria. Purely anechoic/cystic lesions are assigned 0 points, whereas if described as "very hypoechoic" they would be assigned 3 points leading to a likely fruitless FNA and probable patient/physician anxiety.
Frank invasion of surrounding structures is a unfavorable prognostic sign and is assigned 3 points. If minimal extrathyroidal extension is suspected without frank invasion, especially with otherwise benign features, caution and experience should be used when reporting.
Practical points
"Punctate echogenic foci" can encompass both microcalcifications and inspissated colloid, depending on technique and size of the colloid foci in a nodule. Unlike microcalcifications, foci of inspissated colloid are not associated with malignancy and they often appear differently to microcalcifications on closer inspection. Inspissated colloid is not a high risk feature.
Comparison with other classification systems
The ACR system was published in 2017, preceded by K-TIRADS (2017) and followed by EU-TIRADS (2017). Other systems including the ATA and SRU 5 are also in regular use.
Comparative studies show the ACR system has a sensitivity ranging 75-97% and specificity ranging 53-67%, which is either the highest sensitivity and lowest specificity amongst compared systems 6, or, to the contrary, the highest specificity 7,8. With the latter two studies, the ACR system had the greatest overall performance (measured by area under the receiver operating characteristic curve or accuracy), resulting in lower rates of unnecessary fine needle aspiration (false positive rates) 7,8.
Good interobserver agreement regarding decision to biopsy has also been shown (Cohen kappa 0.61) 9.
Revisions
No formal revisions to ACR TI-RADS have been made at present, although one group used artificial intelligence to refine the algorithm, with maintained high sensitivity, increased specificity, and reduced FNA rates 10.
External links
ACR-TI-RADS calculator for thyroid ultrasound (Radcalulators.org)
TIRADS Calculator for Thyroid Nodules (Phillip Cheng, MD MS)
If any of these links are broken or for other problems and questions, please contact editors@radiopaedia.org.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.