
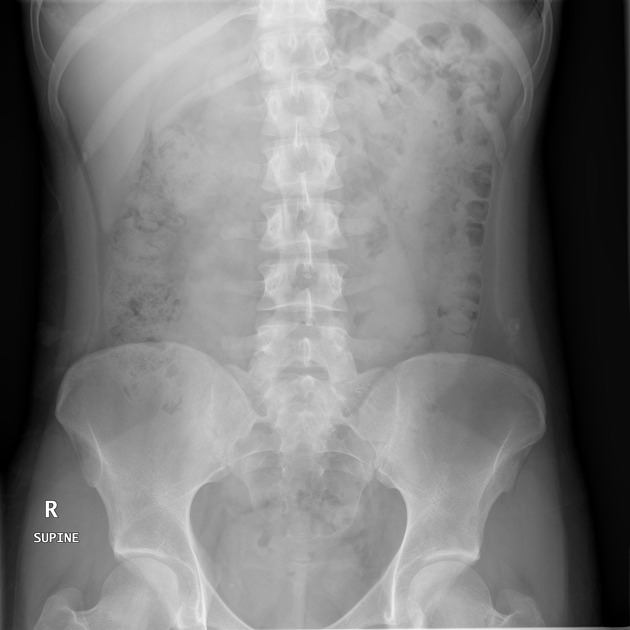
The AP supine abdominal radiograph can be performed as a standalone projection or as part of an acute abdominal series, depending on the clinical question posed, local protocol and the availability of other imaging modalities.
On this page:
Indications
This view is useful in assessing abdominal pathologies, including bowel obstructions, calcifications and neoplastic changes. It is also used as a scout/baseline image for contrast studies of the abdomen (i.e. small bowel follow-through).
Patient position
the patient is supine, lying on his or her back, either on the x-ray table (preferred) or a trolley
patients should be changed into a hospital gown, with radiopaque items removed (e.g. belts, zippers, buttons)
the patient should be free from rotation; both shoulders and hips equidistant from the table/trolley
the x-ray is taken on suspended breathing to prevent motion
Technical factors
AP projection
-
centering point
the midsagittal plane, equidistant from each anterior superior iliac spine (ASIS) at the level of the iliac crest
-
collimation
laterally to the lateral abdominal wall
superior to the diaphragm
inferior to the inferior pubic rami
-
orientation
portrait
-
detector size
35 cm x 43 cm
-
exposure
70-80 kVp
30-120 mAs; AEC should be used if available
-
SID
100 cm
-
grid
yes
Image technical evaluation
if possible, the diaphragm should be included superiorly
-
the abdomen should be free from rotation with symmetry of the:
ribs (superior)
iliac crests (middle)
obturator foramen (inferior)
no blurring of the bowel gas due to respiratory motion
Practical points
For larger patients, it may be necessary to perform two x-rays using a landscape orientation of the detector to include the entire abdomen.
Exposure will need to be adjusted according to the imaging system (CR or DR) and patient size. Where possible, mAs should be manipulated to ensure adequate image density and appropriate image contrast.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.