
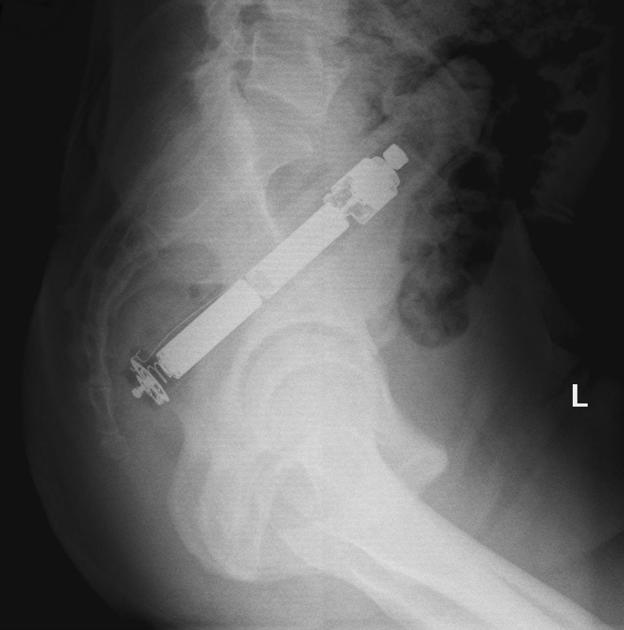
The lateral view abdominal radiograph is a less common projection of the abdomen, it is different from the lateral decubitus view of the abdomen and looks more like a lateral lumbar spine view.
On this page:
Indications
This projection is often requested as a useful problem-solving view that can complement frontal views of the abdomen, often utilized in the context of foreign bodies, to visualize soft tissue masses, umbilical hernia, or prevertebral pathology such as aortic aneurysm or calcifications 2.
This view also better visualize lines such as a shunt (or a part of a dedicated shunt series).
Patient position
the patient may be either erect or recumbent, with her or his side against the detector
legs may be flexed for balance 2
arms raised 2
lower bound of the field of view should contain the inferior pubic ramus
the x-ray is taken in full expiration 2
Technical factors
supine lateral projection
-
centering point
the midcoronal plane at the level of the iliac crest
-
collimation
anterior-posterior to the skin margins
superior to the diaphragm
inferior to the level inferior pubic rami
-
orientation
portrait
-
detector size
35 cm x 43 cm 2
-
exposure
70-80 kVp
30-120 mAs; AEC should be used if available
-
SID
100 cm 2
-
grid
yes
Image technical evaluation
the projection can be confirmed lateral via the lateral appearance of the vertebral bodies
skin border is not burnt out (a filter may be required to address this)
no blurring of the bowel gas due to respiratory motion
Practical points
the lateral abdomen can be useful to visualize rectal gas and differentiate colonic ileus from a distal colonic obstruction however it does not offer much information about bowel gas from the frontal view
this projection can be done erect or supine, often used to localize foreign bodies or as part of a shunt series when there is a high degree of winding of the line



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}