
The anterior oblique projections of the sternoclavicular joints are complimentary to the front on PA view in the sternoclavicular joint series
The side of obliquity pertains to the joint of interest i.e. RAO to assess the right sternoclavicular joint. However, this projection is often performed bilaterally, subsequently, this article will describe the projection as a bilateral examination.
On this page:
Indications
The oblique positioning maneuvers the join of interest away from central structures to produce a clearer view of articulation. It is often requested in the context of significant trauma that can result in sternoclavicular joint dislocation or medial end clavicular fractures. Furthermore, this projection can be requested when following up on already known sternoclavicular injuries in the setting of outpatient appointments.
Patient position
the patient is preferably laid prone with a 10 to 15-degree anterior oblique rotation this is normally achieved with a wedge sponge helping the patient maintain position
a bilateral examination will require the patient to lay RAO and LAO for separate projections
this examination can be performed erect if the patient is stable
Technical factors
posteroanterior anterior oblique projection
-
centering point
centered at the level of the second to third thoracic vertebra at the midline
2-5 cm lateral from the midline toward the raised side (relative to detector i.e. LAO would favor centering laterally towards the right)
-
collimation
laterally to include the medical third of both clavicles
inferior to include the sternoclavicular joints and part of the manubrium
superior to include the entirety of the sternoclavicular joint
-
orientation
landscape
-
detector size
24 cm x 18 cm
-
exposure
60-70 kVp
10-30 mAs
-
SID
100 cm
-
breathing
suspended expiration
-
grid
yes (this can vary departmentally)
Image technical evaluation
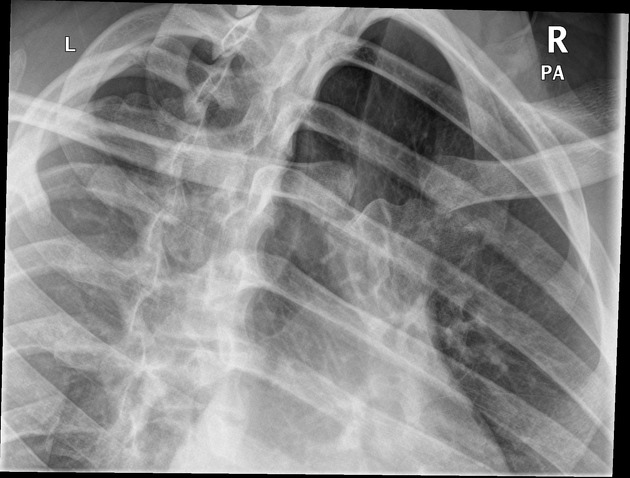
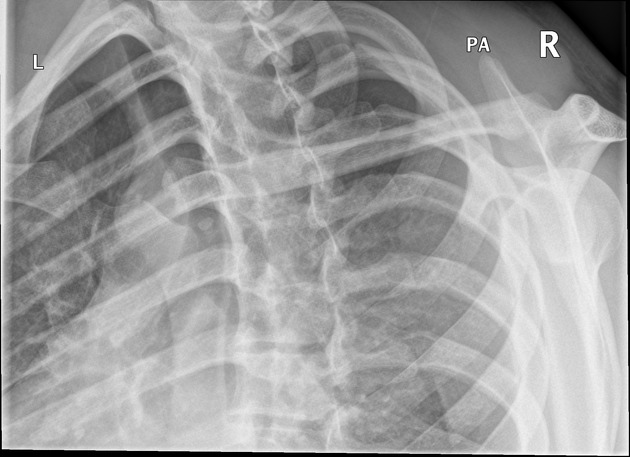
the sternoclavicular joint of interest will be central to the image without foreshortening
the opposite join will appear foreshortened and obscured by the bony thorax
Practical points
the most challenging aspect when performing this projection is collimation; collimation must be tight to avoid scatter thus decreasing the image quality. Time should be taken to ensure the image is collimated appropriately.
-
this projection is often performed bilaterally for comparison, it's important to remember that the side of interest will be the obliquity of the oblique
RAO evaluates the right sternoclavicular joint
LAO evaluates the left sternoclavicular joint
the projection can be performed erect, be wary of the patient's movement


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.