
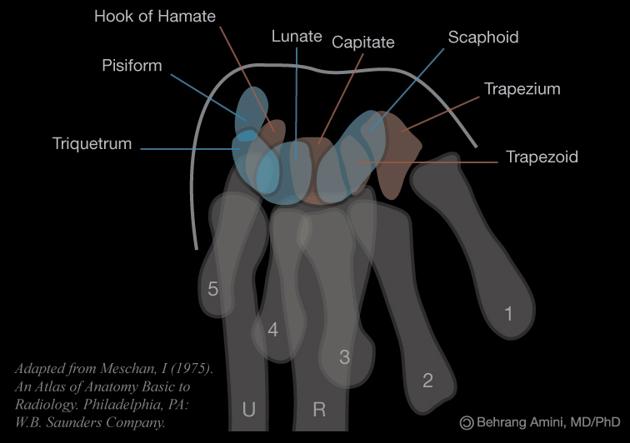
The carpal tunnel view is an axial projection to demonstrate the medial and lateral prominences and the concavity.
On this page:
Indications
This carpal tunnel view is seldom performed however it can be utilized to investigate potential hook of hamate, pisiform and trapezium fractures.
Patient position
- patient stands with the back facing the table
- palmar surface of hand is placed in contact with the cassette which is placed at the table margin
- wrist is dorsiflexed approximately 135º, making the carpals and metacarpals lift away from the cassette
Technical factors
- axial projection
-
centering point
- mid carpal region
- the central ray is vertical and will be centered to the midpoint of the dorsiflexed wrist
-
collimation
- laterally to the skin margins
- dorsal to the skin margins
- ventral to the carpometacarpal joint
-
orientation
- portrait
-
detector size
- 18 cm x 24 cm
-
exposure
- 50-60 kVp
- 3-5 mAs
-
SID
- 100 cm
-
grid
- no
Image technical evaluation
There should be a clear outline of the ventral aspect of the carpal bones with no superimposition.
Practical points
This is a very specialized and slightly outdated projection, yet it is still important to know how to perform it, especially if you don't have a CT scanner readily available.
You can also achieve this projection sitting down, with the hand in forced dorsiflexion; It is often best to ask the patient to pull their fingers back to achieve adequate dorsiflexion, after of course showing them how this is performed. You can then aim the central straight down the carpal tunnel region.
Just remember will cause the significant patient pain if not performed correctly, It is best to demonstrate to the patient physically what you plan to do before making them perform it, this way they are not in discomfort for long.




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.