
Cervical spine lateral view is a lateral projection of the cervical spine.
As technology advances, computed tomography (CT) has replaced this projection. However, many institutions (especially in rural areas) still use it where CT is not readily available.
On this page:
Indications
This projection helps visualize pathology involving the entire cervical spine orthogonal to the AP view. It is often performed in the trauma setting and helps demonstrate any adjacent soft tissue structures, such as osteoarthritis and spondylosis.
Patient position
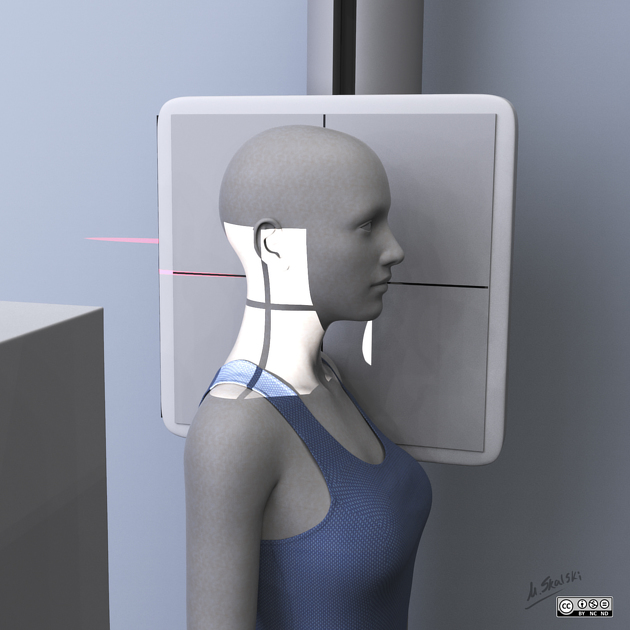
the patient is supine or erect, depending on trauma or follow-up
the detector is placed portrait, running parallel to the long axis of the cervical spine on the patient's left side
inform the patient that the image will be taken on suspended expiration
Technical factors
lateral projection
-
centering point
to a point vertically below the mastoid process (at the level of thyroid cartilage) using the horizontal beam
-
collimation
superior to C1
inferior to T1
anterior to include soft tissue
posterior to the soft tissue
-
orientation
portrait
-
detector size
24 cm x 30 cm
-
exposure
50-75 kVp
20-40 mAs
-
SID
150-180 cm
-
grid
yes
Image technical evaluation
there should be a clear visualization of C1 to T1 (T1 minimum)
the vertebral bodies are superimposed laterally
the articular pillars and zygapophyseal joints are superimposed
Practical points
Traction
this projection may require inferior traction of the arms to better visualize T1, this should only be performed by a qualified individual
-
points to keep in mind whilst traction is being applied:
full expiration is best for optimal inferior displacement of the shoulders to visualize T1
clear communication between yourself and the one performing traction is a must, ensure they are clear when traction is being applied as to avoid motion artifact
ensure individual applying traction is in a lead gown
if T1 cannot be visualized, a swimmer's lateral projection may be required




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.