
The Final FRCR Part B rapid reporting component of the Final FRCR Part B exam is the final part of the FRCR examination. It aims to assess the candidate's ability to accurately detect abnormalities in the type of plain films usually seen in a standard reporting pile. Thus, it generally consists of chest and appendicular radiographs.
Radiopaedia.org Rapids is a set of free practice rapid reporting examinations.
On this page:
Cases
The examination is 35 minutes long and 30 plain films are shown in soft copy using the Royal College of Radiologists digital examination platform, Practique. The candidate must report them as normal or abnormal; where abnormal, they must record the abnormality.
The cases selected by the college examiners must only have one abnormality on them - age-related degenerative change and normal variants are considered "normal".
Of the 30 cases, approximately half will be normal. It is generally considered that when the examiners select cases, they will be more likely to give more abnormal than normal, giving a range of approximately 15-17 abnormal and 13-15 normal. That is just a guide though.
Pass mark
It would appear that there is no clearly defined pass mark. It has previously been said that the pass mark was 26-27/30, but as the marking is adjusted by candidate performance at each sitting, this is difficult to be certain about.
Exam technique
The rapid-reporting exam was previously a test of the candidate's ability to work their way through a packet of hard-copy and much of the exam technique that was banded about related to the difficult of man-handling hard-copy films and keeping track of the films that have been looked at.
What you must not do is spend too long ruminating about the film that is possibly abnormal.
One way of approaching the test
start with the first film
-
is it definitely abnormal?
yes: mark it on the marking sheet and write down what's abnormal
no: move on - do not spend long looking at the film, you will get the chance to do it later
move to the next film - repeat
Using this technique, you should be able to review all 30 films in about 10 minutes and have picked up all the obviously abnormal films. Depending on the test, you might have picked out 10 abnormals in this first run. However, it is worth noting that all radiologists who are not blind will have probably picked out these films too, so they are not discriminatory in the least!
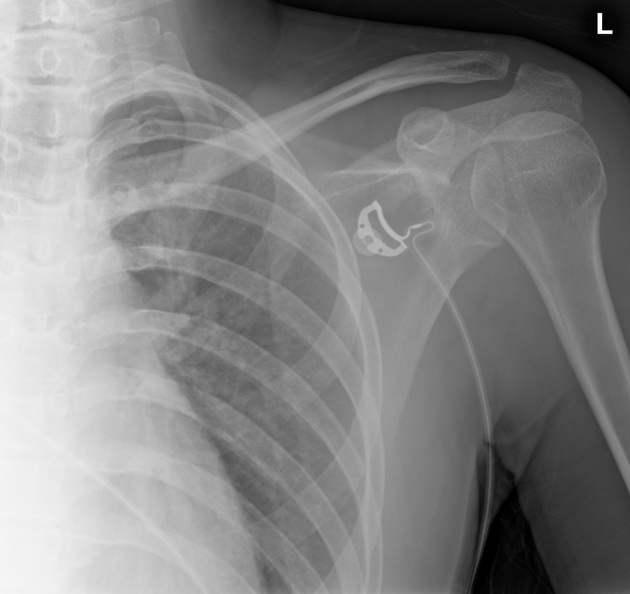
The remaining cases (approximately 20) will contain the remaining 5 or so abnormal films. These will be more subtle and may include pathology located at the edge of the film:
shoulder dislocation on the chest radiograph
dens fracture on the skull radiograph
eroded apical rib
subtle paraspinal collection
fibular fracture only visible on the lateral ankle radiograph through the tibia
subtle pediatric distal radial fracture
The only way to be sure that a film is normal is to have checked it in a systematic fashion to ensure that you have not missed anything. That is where a checklist approach to reporting is helpful - the checklists offered are just a starting point and it will be likely that you will add your review areas.
Alternative approach
Only a few abnormalities can be tested in the exam for each area of the body since only a single image is provided with no clinical information or previous images. Hence, another approach advocated is to be aware of and able to identify a finite list of abnormalities on a plain radiograph for each area of the body.
For example:
-
wrist radiograph
distal radial/ulnar fracture
scaphoid, triquetral, or other carpal bone fracture
metacarpal base fracture
By having a finite diagnostic checklist of abnormalities, you narrow down what you evaluate for on each film. If you think you have identified a possible abnormality that cannot be clearly categorized into your predetermined list, you should strongly consider marking that film as normal. Several lists are available on the range of abnormalities for each body area for the exam.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.