
The suspected foreign body inhalation series aims to detect inhaled foreign bodies or their secondary signs 1. It involves a frontal chest radiograph in both the inspiration and expiratory phases and, in some cases, bilateral-lateral decubitus chest views.
Most inhaled foreign bodies are radiolucent. The absence of a radio-opaque foreign body or secondary signs of inhaled foreign body does not exclude airway obstruction 7. The additional views are intended to demonstrate lung volume that does not change during the respiratory cycle 2. The value of routinely adding these additional views has been questioned in formal study 3,4. Lateral decubitus views may increase false positives without increasing true positives 4. This is a particular issue for children where management subsequently involves bronchoscopy under general anesthesia. Adding an expiration phase view increases true positives without increasing false positives, but accuracy is not high, calling clinical utility of this additional exposure into question 4.
Low dose CT chest has been suggested as a subsequent investigation to radiographs in stable patients with suspected radiolucent foreign body aspiration, as it can accurately identify clear airways that do not need bronchoscopy, or direct bronchoscopy to the affected airway(s) 5,6. An ultralow dose CT chest protocol for foreign body aspiration evaluation in children was shown to have a lower effective dose, and both better sensitivity and specificity, than a standard foreign body radiograph protocol making it the investigation of choice, if available 8.
On this page:
Patient position
Patient positioning will depend on patient age. The frontal chest radiograph can be performed erect or supine, conditional to the patients’ needs. The lateral decubitus radiographs will follow the same position advice as to the lateral decubitus view.
Technical factors
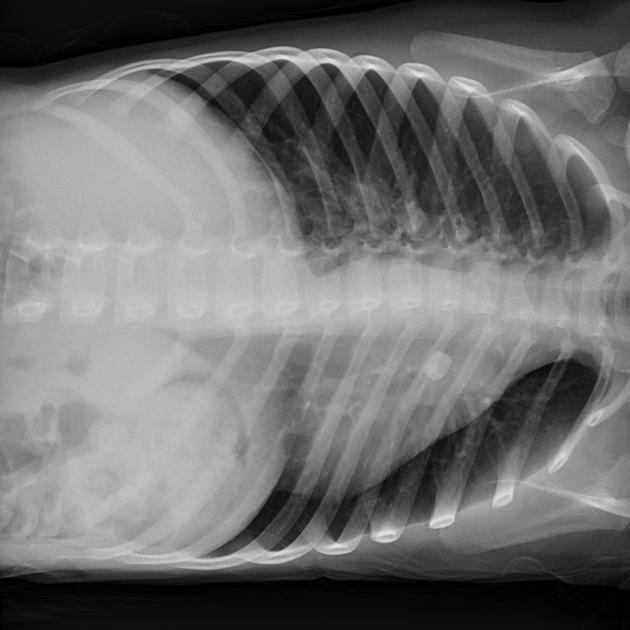
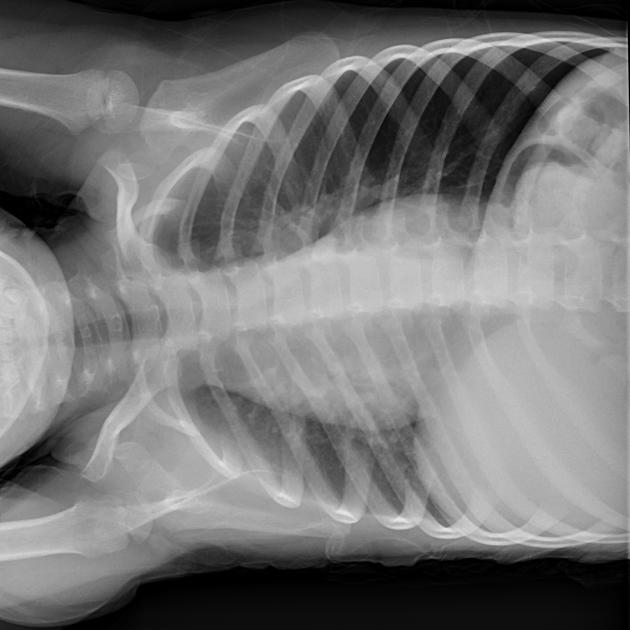
chest inspiration and expiration
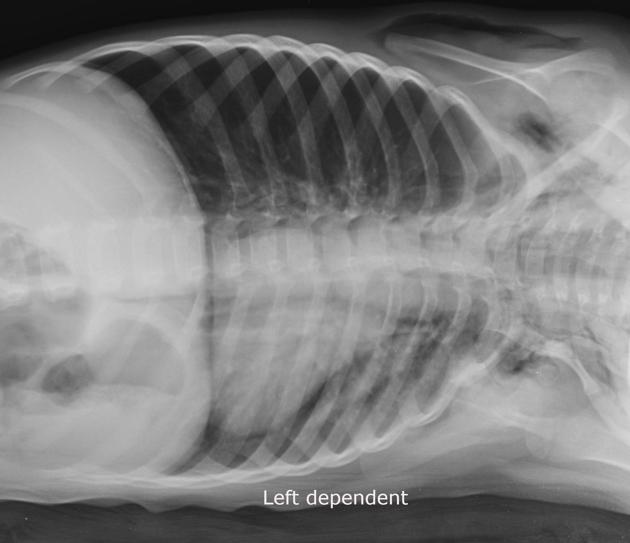
bilateral lateral decubitus
Image technical evaluation
-
entire lung fields should be visible; post-processing collimation is not advisable in pediatric imaging (if it is exposed it should be examined).
-
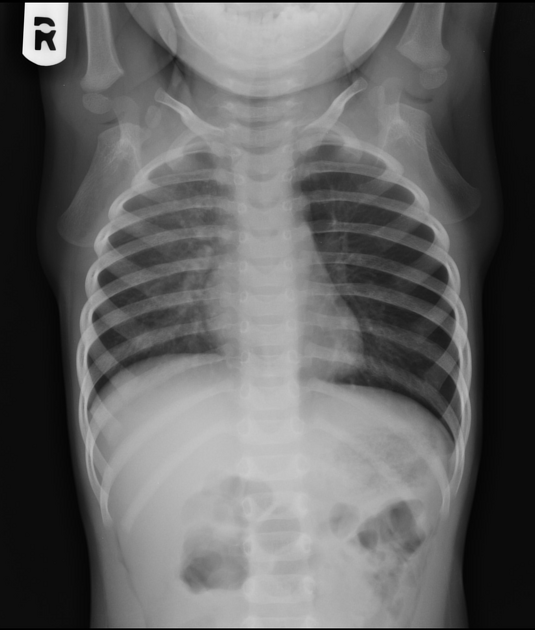
full inspiratory effort
ensure 8 visible posterior ribs in children aged 0-3 years old
ensure 9 posterior ribs in children aged 3-7 years old
ensure 10 posterior ribs in children aged 7 years old and above
-
due to ossification centers in children, the medial ends of clavicles are difficult to visualize; therefore measuring the medial ends of the clavicle to the spinous process is not advised
the head of clavicles to lie at the level between T2 and T4
Practical points
it is important to obtain a true inspiration and expiration radiograph as this will better demonstrate the secondary signs of the ball-valve phenomenon evident in inhaled foreign bodies
bilateral decubitus views should demonstrate hyperinflation of the affected lung on both radiographs; in the obstructive foreign body there will be air-trapping and therefore hyperlucency of the dependent lung


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.