
The AP view of the humerus is part of the humerus series and is usually taken in a standing position. However, it can also be obtained in a supine position.
The projection demonstrates the humerus in its natural anatomical position allowing for adequate radiographic examination of the entire humerus and its respective articulations.
On this page:
Indications
Humerus views are often done to exclude large humeral shaft fractures or suspected symptomatic metastatic lesions 1. If an occult fracture is suspected at either the proximal or distal end, it is best to do a separate elbow or shoulder series.
Patient position
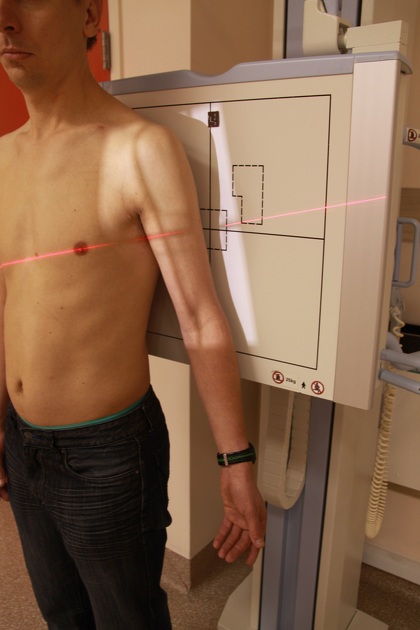
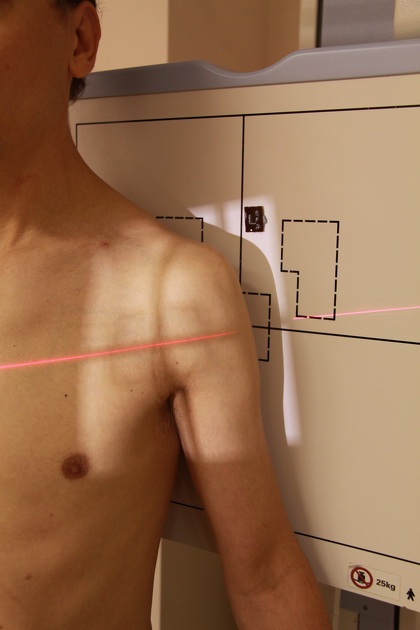
the patient is preferably erect
the patient's back is against the image receptor
the affected arm is abducted and centered to the upright detector, if possible, the arm is slightly externally rotated to mimic the true anatomical position
Technical factors
anteroposterior projection
-
centering point
mid humerus shaft
-
collimation
superior to the skin margins above the glenohumeral joint
inferior to include the distal humerus including the elbow joint
lateral to include the skin margin
medial to include skin margin
-
orientation
portrait
-
detector size
35 cm x 43 cm
-
exposure
60-70 kVp
7-15 mAs
-
SID
100 cm
-
grid
yes (this can vary departmentally)
Image technical evaluation
The humerus is positioned AP, evidenced by the medial and lateral epicondyles seen in profile and the greater tubercle being seen on the lateral aspect of the humerus. The shaft is abducted away from the patient's body, minimizing superimposition
Practical points
It is best to show the patient how you want their arm to rest for the projection. Often, you will have to rotate the light beam diaphragm to be aligned with the long axis of the humerus.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.