
The knee anteroposterior view is a standard projection to assess the knee joint, distal femur, proximal tibia and fibula and the patella.
On this page:
Indications
This view demonstrates the distal femur and proximal tibia/fibula in their natural anatomical position allowing for assessment of suspected dislocations, fractures, localizing foreign bodies and osteoarthritis.
Patient position
patient is supine on the table with the knee and ankle joint in contact with the table
leg is extended
ensure the knee is not rotated
Technical factors
anteroposterior projection
-
centering point
center of the knee 1.5 cm distal to the apex of the patella
-
collimation
superior to include the distal femur
inferior to include the proximal tibia/fibula
lateral to include the skin margin
medial to include medial skin margin
-
orientation
portrait
-
detector size
24 cm x 30 cm
-
exposure
60-70 kVp
7-10 mAs
-
SID
100 cm
-
grid
no
Image technical evaluation
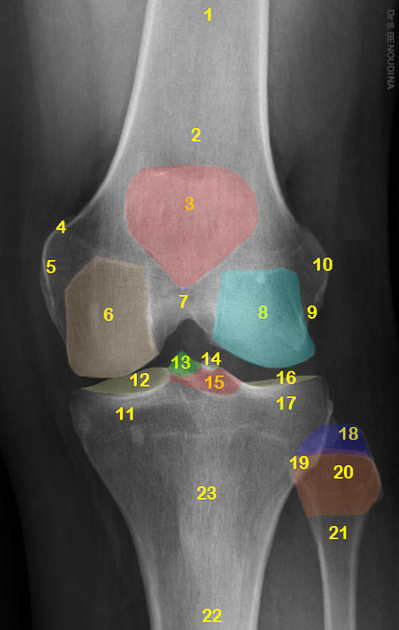
The femoral and tibial condyles should be symmetrical, with the head of the fibula slightly superimposed by the lateral tibial condyle. The patella is resting on the superior portion of the image superimposing the distal femur.
Practical points
The fibula head is a great indication of rotation, if the fibula head is entirely superimposed, the image is not AP; to correct this you must internally rotate until the knee is in even contact with the image detector.
Very slim patients may require a slight caudal angle to better visualize the joint space in an AP fashion. The opposite applies for larger patients (thicker thighs mean the leg may be naturally flexed at rest) and would require a slight cephalic angle. Whether cephalic or caudal, an angle of approximately 5-8° is adequate.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.