
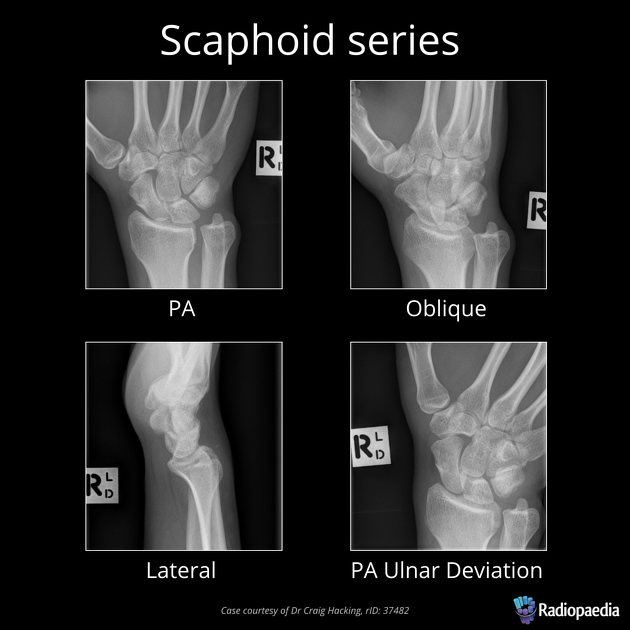
The scaphoid series is comprised of posteroanterior, oblique, lateral and angled posteroanterior projections. The series examines the carpal bones focussed mainly on the scaphoid. It also examines the radiocarpal and distal radioulnar joints along with the distal radius and ulna. Scaphoid fractures are often a result of FOOSH injuries and have a bad prognosis if missed (risk of avascular necrosis of proximal aspect in scaphoid waist fracture). Often if a scaphoid fracture is suspected and not seen on plain film, a follow-up will be performed in 7-10 days 1.
Indications
Scaphoid x-rays are indicated for a variety of settings including:
bony tenderness at the anatomical snuffbox
suspected fracture
obvious deformity
Projections
Standard projections
-
ulnar deviation to remove the scaphoid from the radius and present its axis longitudinally
the best view to inspect the joint spaces of the carpal bones and the distal radioulnar joint
-
ulnar deviation to remove the scaphoid from the radius and present its axis longitudinally
tube angulation to present the scaphoid en face
-
external oblique projection
-
projection 90° to the PA view
demonstrates multiple carpal bones overlapping
the essential view to assessing the alignment of the radius, lunate, and capitate in the setting of a suspected dislocation
Modified trauma projections
-
modified lateral projection that requires little to no patient movement
produces a diagnostic lateral projection without risking patient pain
Additional projections
-
used for suspected scapholunate dissociation



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.