
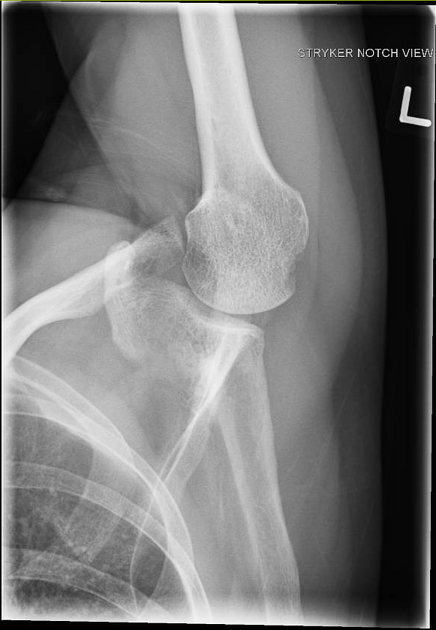
The Stryker notch view is a specialized projection of the shoulder, aimed at assessing the posterior humerus.
On this page:
Indications
The Stryker notch view can be used post anterior glenohumeral dislocation, assessing for Hill-Sachs defects 1.
Patient position
- the patient is preferably erect
- the mid-coronal plane of the patient is parallel to the image receptor: the patient's back is against the image receptor
- the glenohumeral joint of the affected side is at the center of the image receptor
- the patient is turned toward the affected side to show the glenohumeral joint space; this is achieved by rotating the patient 30-45°
- affected arm is abducted anteriorly and rested on the patient's head while maintaining internal rotation (if possible)
Technical factors
- anteroposterior inferosuperior axial projection
-
centering point
- 10-15° cephalad angle of the x-ray tube
- mid-axilla at the level of the glenohumeral joint
-
collimation
- superior to include the entire neck of the humerus
- inferior to include the glenoid
- lateral to the extent of the humeral head
- medial to the extent of the humeral head
-
orientation
- portrait
-
detector size
- 18 cm x 24 cm
-
exposure
- 60-70 kVp
- 10-18 mAs
-
SID
- 100 cm
-
grid
- yes (this can vary departmentally)
Image technical evaluation
- the glenohumeral joint should be open
- the humerus is pointing superiorly
- the lateral portion of the humeral head should be free from any superimposition
Practical points
- it is important to demonstrate to the patient how this projection needs to be performed
- set the patient up (similar to an AP glenoid projection), then ask the patient to abduct the arm and place it on their head
- tight collimation avoids any unwanted scatter
- rotation of the patient will vary due to body habitus: this is an obvious point but highly relevant
- patients who require these films are often suffering from either chronic or acute shoulder pain and palpating the affected shoulder is far from ideal
- it is advisable to observe the clavicle when rotating the patient until the midshaft of the clavicle is almost end on




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.