
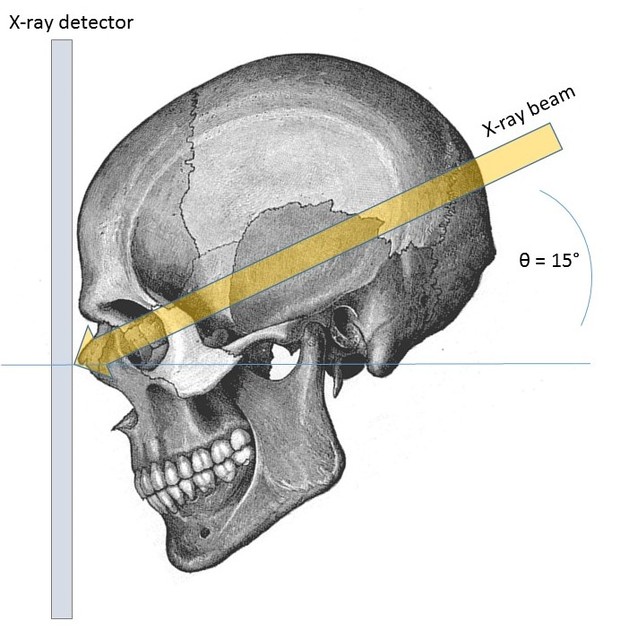
The Caldwell view is a caudally angled radiograph, with its posteroanterior projection allowing for minimal radiation to the orbits. This view may be used in imaging of the skull or facial bones depending on the clinical indications.
On this page:
Indications
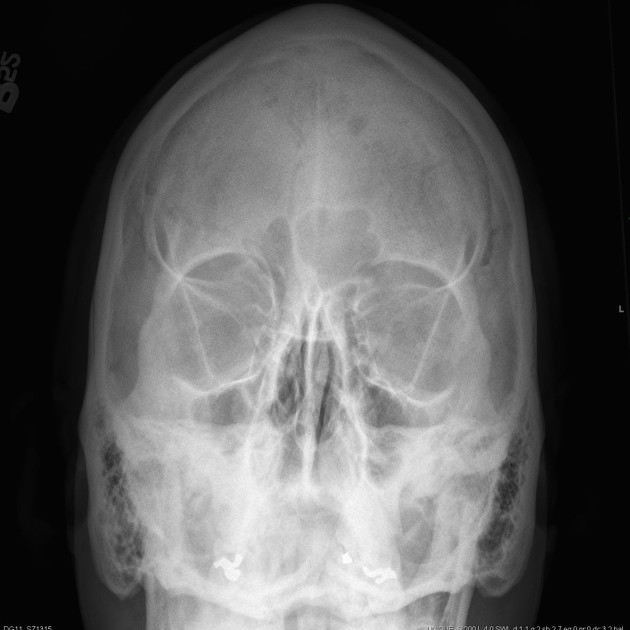
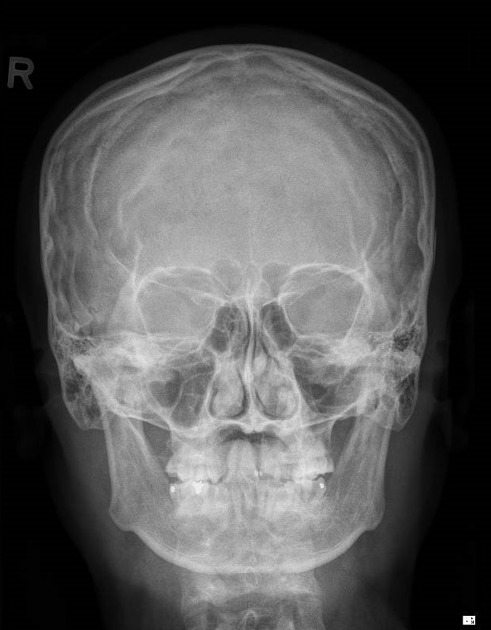
This view aids in visualizing the paranasal sinuses, especially the frontal sinus 4. It can help to assess inflammatory conditions such as sinusitis and secondary osteomyelitis, and sinus polyps or cysts.
Additionally, skull fractures, neoplastic processes, or Paget disease may also be visualized via this view 4.
Patient position
the patient is seated in front of the upright detector
the patient's forehead is placed against the image detector 4
forehead and nose are both touching the detector
the orbitomeatal line (OML) is running perpendicular to the detector
petrous ridge is below orbits 4
Technical factors
posteroanterior (PA) projection
-
centering point
angled caudad around 15° to exit at the nasion
-
collimation
lateral to the skin margins
superior and inferior to the borders of the sinus cavities
-
orientation
portrait
-
detector size
24 cm x 30 cm 4
-
exposure
70-80 kVp 4
20 mAs
-
SID
100 cm 4
-
grid
yes 4
Image technical evaluation
no rotation evident via the symmetrical nature of the orbits
the innominate lines should be equidistant from the lateral borders of the orbits
petrous ridges are projected in the lower third of the orbits
no tilting should be evident; an imaginary line through the petrous ridges should be horizontal 4
Practical points
always guarantee that the patient is not 'hunched' over when they are being examined. This can cause an artifact from the shoulders and the patient is more likely to be rotated; it is best to move the chair up close to the detector so they are sitting up straight for the image
remember, having one's head against an upright detector is uncomfortable, so try to have everything set up before you position the patient, to ensure patient comfort
constantly use a side marker and regularly place it PA. Skulls can get tricky with figuring out which side is which. Many vendors tend to 'flip' images to make them appear AP
alternative projections at 25° to 30° are for better visualization of superior orbital fissures, foramen rotundum, and inferior orbital rim 4.
for those trauma patients that are unable to position for PA projection, an AP projection can be used with 15° cephalic angle and orbital-meatal line position perpendicular to image receptor (IR) 4
History and etymology
The view was first described by Eugene Wilson Caldwell in 1907 3, an American radiologist.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.