
The serendipity view is a specialized radiographic projection utilized in the setting of suspect dislocations of the sternoclavicular joint. The projection is seldom used in departments with functioning computed tomography, but still utilized in postoperative imaging.
On this page:
Indications
The serendipity view is often requested in the context of significant trauma that can result in sternoclavicular joint dislocation or medial end clavicular fractures. Furthermore, this projection can be requested when following up on already-known sternoclavicular injuries in the setting of outpatient appointments.
Patient position
supine on the radiographic examination table
Technical factors
axial projection
-
centering point
at the level of the sternoclavicular joint with a 40-degree cephalic angle
-
collimation
laterally to include the medial third of both clavicles
inferiorly to include the sternoclavicular joints and part of the manubrium
superiorly to include the entirety of the sternoclavicular joint
-
orientation
landscape
-
detector size
24 cm x 18 cm
-
exposure
60-70 kVp
10-30 mAs
-
SID
100 cm
-
breathing
suspended expiration
-
grid
yes (this can vary departmentally)
Image technical evaluation
both sternoclavicular joints are clearly evident
sharp bony detail
no evidence of motion
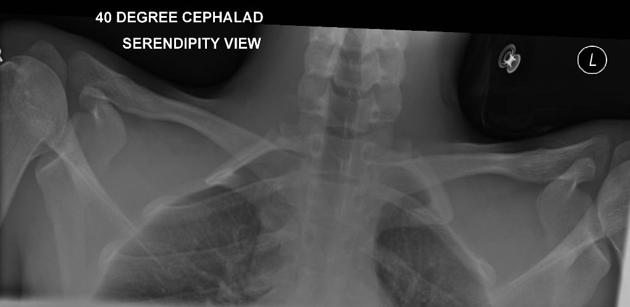
use of appropriate angle evident via clear bony structures free from excessive distortion, an example of too much angle and inadequate collimation can be seen in figure 1
-
normal anatomy 1
the medial ends of the clavicle are equal distance apart in the same horizontal plane
-
posterior dislocation 1
the medial end of the dislocated clavicle will be inferior to the mean horizontal plane of the sternoclavicular joint
-
anterior dislocation 1
the medial end of the dislocated clavicle will be superior to the mean horizontal plane of the sternoclavicular joint (figure 2)
Practical points
This projection is rarely practised; consequently, it is regarded as an advanced radiographic investigation. The most challenging part of the examination is ensuring your patient is supine on the correct portion of the table to allow adequate room to line up the detector to the tube.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.