
The lateral elbow view is part of the two view elbow series, examining the distal humerus, proximal radius and ulna. It is deceptively one of the more technically demanding projections in radiography 1-3.
The projection is the orthogonal view of the AP elbow allowing for examination of the ulna-trochlear joint, coronoid process, and the olecranon process. It is used to assess both the anterior humeral and the radiocapitellar line.
On this page:
Indications
This view is clinically indicated for trauma to, chronic discomfort or infection of the elbow joint. It aids in visualizing fractures and/or dislocations to any articulating bones of the elbow joint, in addition to osteomyelitic and arthritic changes.
The visualization of the posterior fat pad sign on a true lateral projection indicates an elbow joint effusion and is suggestive of an occult fracture if no obvious fracture is seen. The sail sign or the triangular appearance of the elevated anterior fat pad should also raise suspicions of an occult fracture.
Patient position
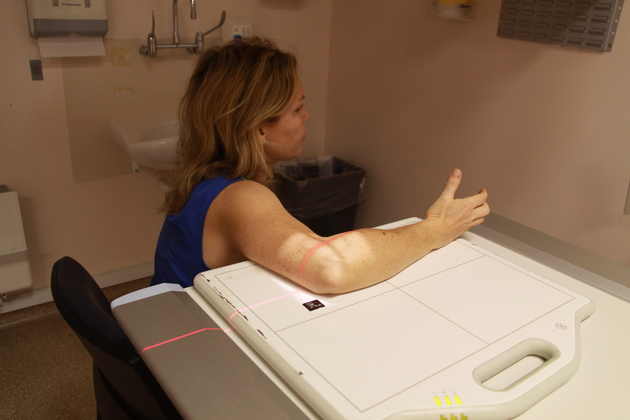
patient is sitting next to the table
at 90 degrees elbow flexion, the medial border of the palm and forearm are kept in contact with the tabletop (see figures 1-3)
the shoulder, elbow and wrist are kept in the same horizontal plane (see figure 1)
rotate the hand so the thumb is pointing towards the ceiling, ensuring all aspects of the arm from the wrist to the humerus are in the same plane
Technical factors
lateral projection
-
centering point
lateral epicondyle of the humerus
-
collimation
superior to distal third of the humerus
inferior to include one-third of the proximal radius and ulna
anterior to include the skin margin
posterior to skin margin
-
orientation
landscape
-
detector size
18 cm x 24 cm
-
exposure
50-60 kVp
2-5 mAs
-
SID
100 cm
-
grid
no
Image technical evaluation
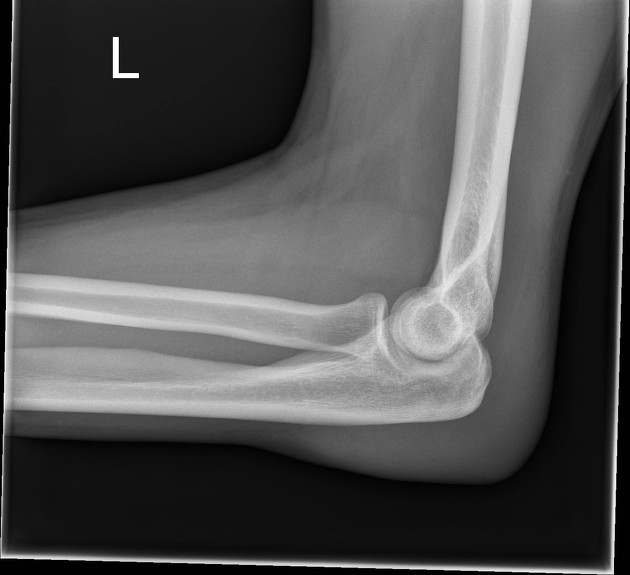
medial epicondyle is superimposed over the anterior third of the distal humerus, rather than dead center
there is a superimposed, concentric relationship of the trochlear groove (smallest circle) and the medial lip of the trochlea with the capitellum
olecranon process is visible in profile
elbow joint is open
radial tuberosity is superimposed and not in profile (indicating the arm is not pronated)
Practical points
It is worth learning the anatomical and radiological appearances of the capitellum, trochlea and the medial epicondyle to assess the optimal lateral elbow. An excellent tool for identifying the capitellar is making use of the radiocapitellar line, the middle of the radial head transects the capitellum unless there is pathology such as a dislocation.
The AP projection of the elbow will show the radial tuberosity in profile, to get a lateral view of the proximal radius it is important to have the forearm halfway between supination and pronation (thumb pointing up).
The radial tuberosity should be superimposed.
Positional errors
-
capitellum protruding posteriorly
the hand is sitting 'too high' and is typically corrected if you lower the hand.
-
capitellum protruding anteriorly
external rotation is evident via the capitellum is projecting anteriorly in addition to the medial condyle moving posterior, creating a double concave like protuberance. That is alleviated via placing the side in questions arm on a small foam block, essentially raising the hand to ensure all aspects of the upper limb are in the same plane.
-
capitellum protruding inferiorly
the elbow/table must be raised
-
capitellum protruding superior
the elbow/table must be lowered













 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.