
Immunodeficiency-associated CNS lymphomas are recognized in the WHO classification of CNS tumors (2021, 5th edition) as one of the distinct diagnoses nested within primary CNS lymphomas. Within this diagnosis are a number of entities previously recognized as separate entities, all of which share immunocompromised hosts, large B-cell morphology and are EBV-related.
On this page:
Terminology
In previous WHO classifications, and therefore still widely seen in the literature, are a number of specific diagnoses that no longer warrant their own diagnosis but what are, nonetheless, worth discussing individually as they occur in distinct clinical contexts. These include:
Epidemiology
Essentially any cause of immunosuppression increases the risk of developing a primary CNS lymphoma. These include 1:
-
iatrogenic immunodeficiency, e.g.
azathioprine
methotrexate
mycophenolate
-
congenital immunodeficiency syndromes, e.g.
-
acquired immunodeficiency syndromes, e.g.
HTLV
-
autoimmune diseases, e.g.
senescence
As such the epidemiology will reflect those of the underlying condition/cause and will vary from region to region. Overall, immunodeficiency-associated CNS lymphomas account for 8-10% of all lymphomas 2.
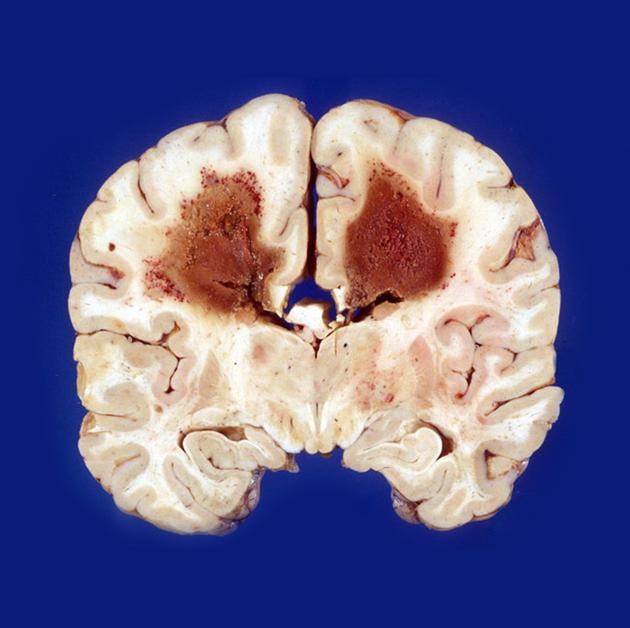
Pathology
Immunodeficiency-associated CNS lymphomas are of B-cell origin and therefore have the usual B-cell markets (CD19, CD20 and CD79a). In most instances, and unlike sporadic primary CNS lymphomas, these tumors are associated with prior EBV infection 1.
They express EBER1, EBER2, LMP1 and EBNA1-6 1.
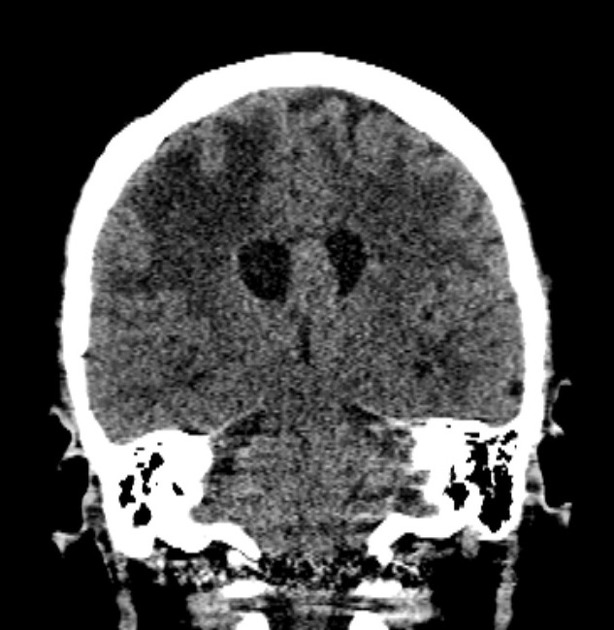
Radiographic features
Although generally, the features of immunodeficiency-associated CNS lymphomas is similar to that of sporadic primary diffuse large B-cell CNS lymphoma, in the setting of immunodeficiency tumors are far more likely to demonstrate 1,2:
heterogeneous signal
peripheral enhancement with central non-enhancement due to necrosis
multifocality
surrounded by a greater degree of vasogenic edema
It is important to note, however, these findings are far from pathognomonic for immunodeficiency, and are seen, albeit less frequently, in immunocompetent primary diffuse large B-cell lymphoma of the CNS.
Treatment and prognosis
The combination of immunosuppression/immunodeficiency and an aggressive tumor, immunodeficiency-associated CNS lymphomas generally carries a poor prognosis 1.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.