
Transposition of the great arteries (TGA), also known as transposition of the great vessels (TGV), is the most common cyanotic congenital cardiac anomaly presenting during the newborn period, with cyanosis in the first 24 hours of life.
It occurs as a result of ventriculoarterial discordance, with the aorta arising from the right ventricle and the pulmonary trunk from the left ventricle. It can be subdivided into two main types depending on the positional relationship of the aortic valve with the pulmonary valve:
L-loop transposition of the great arteries: congenitally corrected TGA
D-loop transposition of the great arteries (this article mainly focuses on the D-loop transposition).
On this page:
Epidemiology
Transposition of the great arteries accounts for up to 7% of all congenital cardiac anomalies 1, with an estimated incidence of ~1 in 5000 births. It is an isolated abnormality in 90% of those affected and rarely is associated with a syndrome or an extra-cardiac malformation. It is most common in infants of diabetic mothers 1.
Associations
Approximately 90% occur as an isolated finding, and extracardiac syndromic associations are rare. Associations have been described with:
maternal diabetes
-
congenital coronary arterial anomalies
most common anomalous origin involves the left circumflex arising from the right coronary artery
single (right or left) coronary arteries
inverted coronary origins
Clinical presentation
The majority of neonates do not carry the diagnosis at birth, discovered in about 10% of cases. The vast majority of patients are then diagnosed between the first day and end of the first week of life with marked central cyanosis without respiratory distress; this includes those patients with an intact ventricular septum and those with a combination of a ventricular septal defect and concomitant left ventricular outflow tract obstruction.
Those who have a large, nonrestrictive ventricular septal defect will be perhaps only mildly cyanotic during exertion and tend to present after a few weeks with symptoms of heart failure, such as:
diaphoresis
irritability
poor weight gain
decreased activity levels
Physical examination may reveal a right ventricular heave, a thrill at the left lower sternal border, and if left ventricular outflow tract obstruction is present a systolic murmur at the upper sternal border may be appreciated. A pathognomonic feature, albeit rare, on the physical exam would be cyanosis manifest in the upper extremities with normal-appearing, acyanotic lower extremities. This is referred to as reverse differential cyanosis, and will only occur in dextro-transposition which coexists with a patent ductus arteriosus as well as either an interrupted aortic arch or coarctation of the aorta.
Pathology
Transposition of the great arteries occurs as a result of ventriculoarterial discordance, with the aorta arising from the right ventricle and the pulmonary trunk from the left ventricle. It can be subdivided into two main types depending on the positional relationship of the aortic valve with the pulmonary valve:
L-loop transposition of the great arteries: congenitally corrected TGA
D-loop transposition of the great arteries
An isolated TGA is incompatible with life at birth without one of the following additional anomalies (which are a common occurrence 2):
atrial septal defect (ASD): uncommon
patent ductus arteriosus (PDA): unstable due to closure following birth
patent foramen ovale (PFO): unstable
Unstable associations account for 60-65% of occurrences.
Radiographic features
Plain radiograph
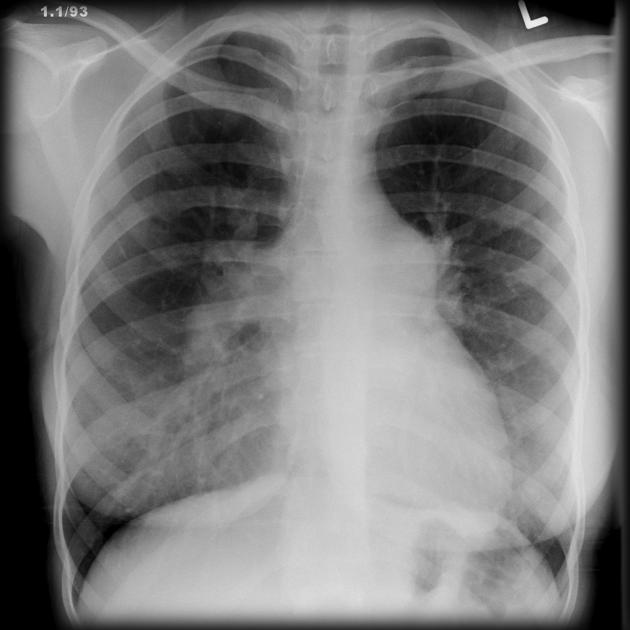
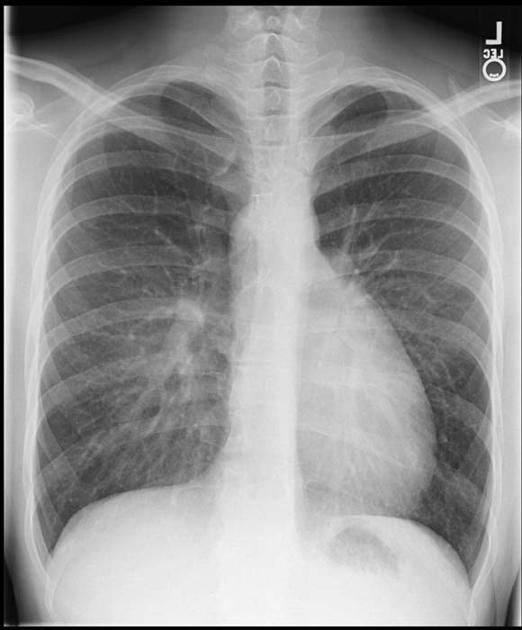
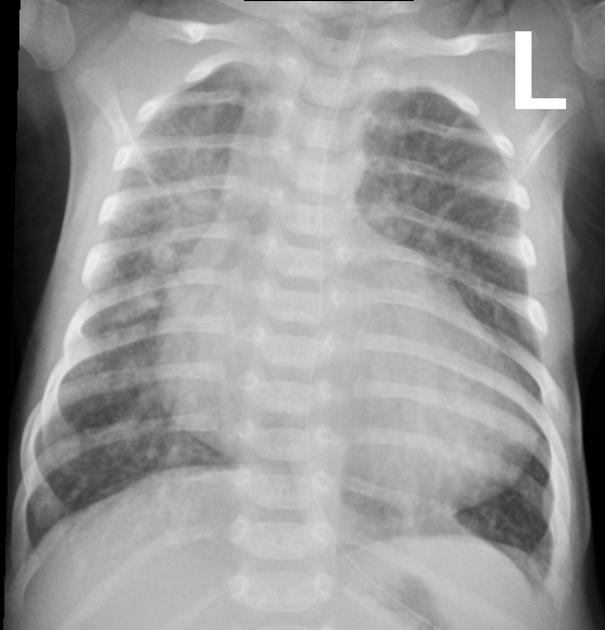
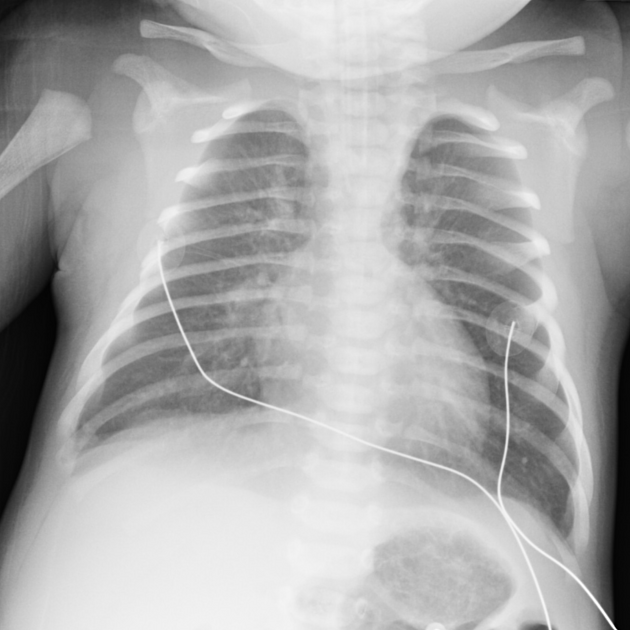
A frontal chest radiograph classically shows cardiomegaly with cardiac contours classically described as appearing like an egg on string 1. There is often an apparent narrowing of the superior mediastinum as the result of the aortic and pulmonary arterial configuration, i.e. parallel in D-loop transposition, with the main pulmonary artery posterior to the aorta.
Ultrasound
Fetal echocardiography
Allows direct visualization of abnormal anatomy with the aorta and pulmonary trunk lying in parallel with an absence of crossing (best seen in the base view of the fetal heart) 4.
Transthoracic echocardiography
-
parasternal long axis view allows visualization of the great vessels traveling in parallel
main pulmonary artery conspicuous as it branches posteriorly from the left ventricle and bifurcates into branch pulmonary arteries
the aorta may be visualized anteriorly in the near field originating from the right ventricle 9
-
short axis views at the great vessels allow delineation of the spatial relationship between the great vessels and the coronary artery origins
in the most common orientation, the aorta will be anterior and slightly to the right of the pulmonary artery
color flow Doppler may enhance the visualization of the orientation of the coronary ostia
the origin of the left coronary commonly arises from the left anterior facing sinus of Valsalva, and the origin of the right coronary artery from the left posterior facing 11
-
apical views can likewise confirm ventriculoarterial discordance with anteroposterior inspection of the origin and course of the great vessels
also useful to evaluate the degree of outflow tract obstruction present given the commonly present subaortic infundibulum between the tricuspid and aortic valves
fibrous continuity between the mitral and pulmonary valves present
leftward septal bowing from right ventricular pressure overload may result in dynamic left ventricular outflow tract obstruction (LVOTO) 12
the suprasternal sagittal view is optimal to visualize the patent ductus arteriosus (PDA) as well as determining the direction and relative amount of shunting
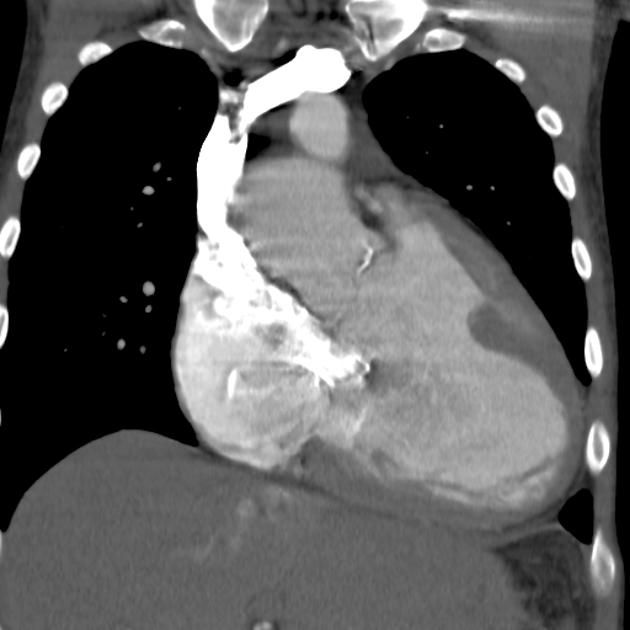
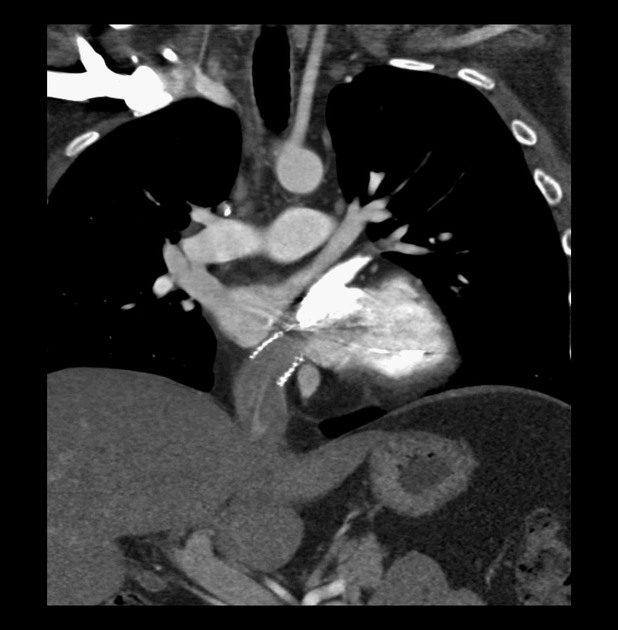
CT/CTA
Allows direct visualization of abnormal great vessel anatomy. Cardiac-gated cine CT can additionally assess function.
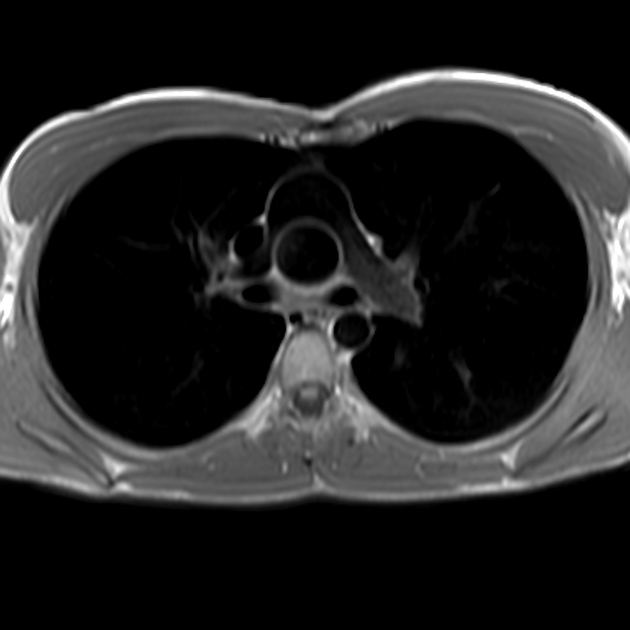
MRI
Cardiac MRI allows direct visualization of abnormal anatomy. SSFP cine sequences can additionally determine flow dynamics.
Treatment and prognosis
Initial Rashkind septoplasty is usually done as a palliative procedure in neonates.
Previously TGAs were definitively surgically corrected with atrial switch operations, such as a Mustard repair or Senning repair, which have been superseded by arterial switch procedures 5.







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.