
Computed tomographic (CT) colonography, also called CTC, virtual colonoscopy (VC) or CT pneumocolon, is a powerful minimally invasive technique for colorectal cancer screening.
On this page:
Indications
screening test for colorectal carcinoma
colon evaluation after incomplete or unsuccessful optical (conventional) colonoscopy
assessment of strictures
to better evaluate the colon proximal to obstructing neoplasms detected by conventional colonoscopy
patients with contraindications to or refusing optical colonoscopy
Technique
-
patient preparation
for optimal image quality, the colon should be clean and completely distended
residual stool and fluid may lead to a false negative or false positive diagnosis
residual stool may be "tagged" using oral contrast agents such as Gastrografin
-
bowel distension
optimal colonic distention is critical to technical success for proper intraluminal evaluation of the large bowel
distension can be achieved via a pressure-regulated device with carbon dioxide (preferred) or room air
-
intravenous contrast
not necessary for colonic interpretation although it is used in some centers for better assessment of the remaining abdominal organs
if used, the time difference between scanning in supine and prone positions means the first acquisition may be portal venous, but the second acquisition will be a more excretory (urographic) phase
-
antispasmodic agent
IV/IM hyoscine-N-butylbromide (Buscopan), an antimuscarinic drug reduces colonic motion, leading to higher quality images and reduced patient discomfort
IV glucagon is used in some countries/institutions as a first or second-line antiperistaltic agent: its efficacy is contentious
Data acquisition and analysis
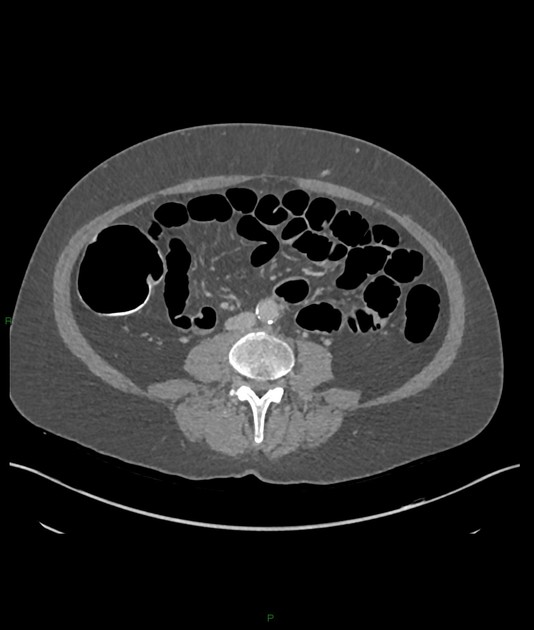
CT scanning is ideally performed on a multidetector computed tomography (MDCT) scanner in both supine and prone positions with a thin collimation
slice thickness of CT colonography may range from 1.25 mm to 5 mm 8
CT colonography may detect polyps size from 2 mm or larger, however, the significance of detecting polyps less than 5 mm is of questionable clinical significance 8
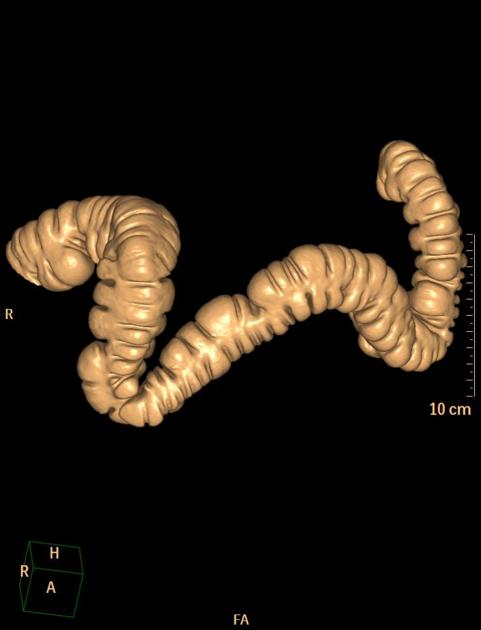
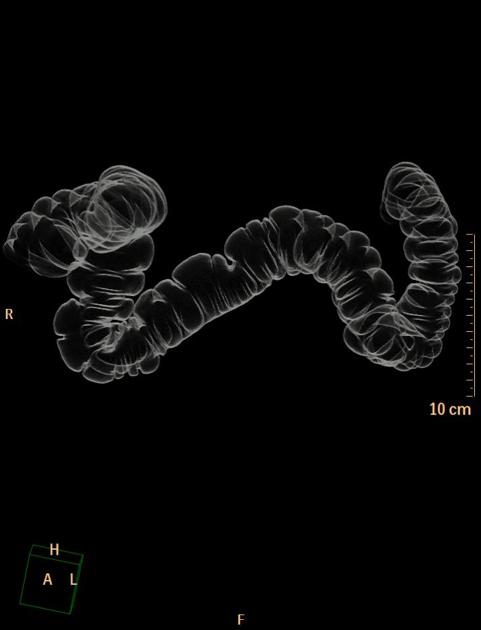
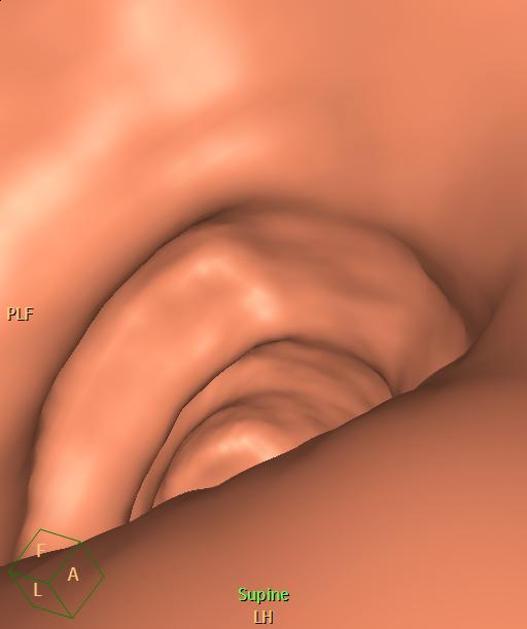
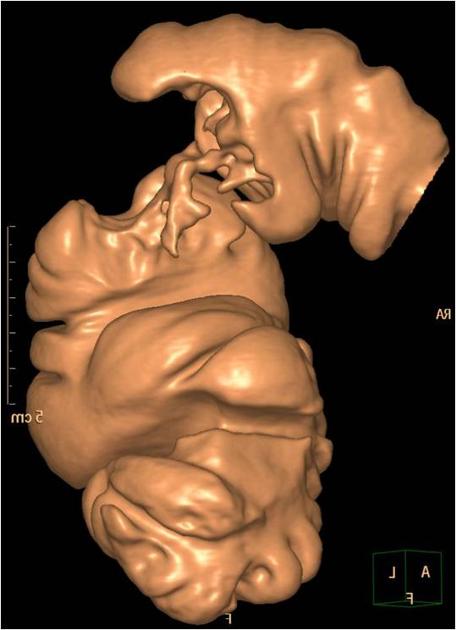
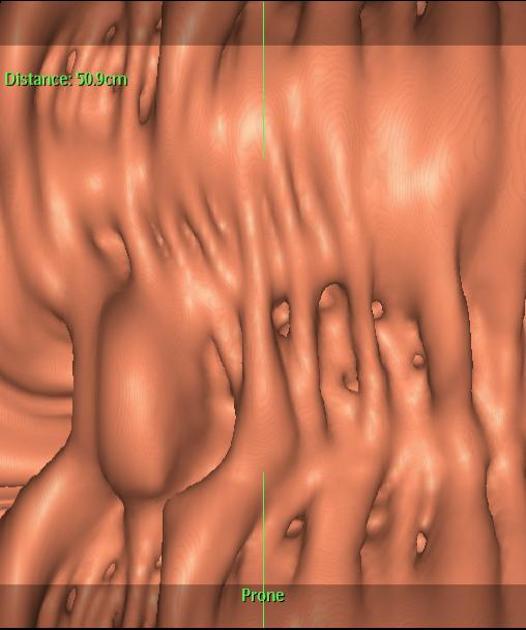
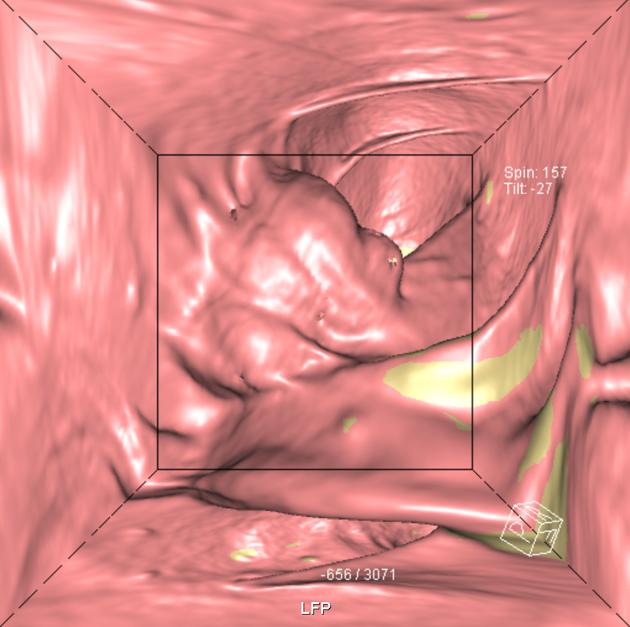
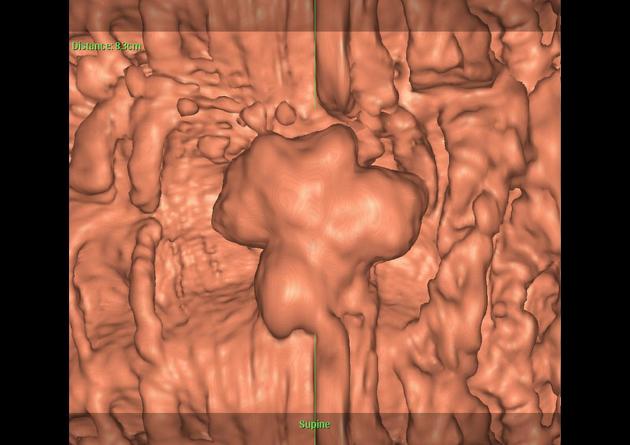
image review with the use of two-dimensional (2D) and three-dimensional (3D) displays is strongly advised for optimal evaluation
Findings
extrinsic lesions impressing on the colon
extracolonic pathology
Contraindications
Absolute
acute inflammatory conditions such as acute diverticulitis, active stage of ulcerative colitis or Crohn disease
recent abdominal or pelvic surgery
Relative
CTC more difficult to perform if a colostomy is present as there is no natural sphincter mechanism to retain the gas
general CT contraindications e.g. pregnancy, claustrophobia, etc.
-
history of severe adverse reaction/anaphylaxis to iodinated contrast media
protocols using barium sulfate contrast media may be used as an alternative
patients at high risk for a gastrointestinal tumor (e.g. Lynch syndrome) may not be good candidates for CTC screening 7
Complications
Bowel perforation is very rare following CT colonography but nevertheless is well-recognized as a potential complication with rates from 0.005% to 0.03% 9. The risk of perforation seems to be higher when 9,10:
pre-existing obstructive bowel pathology including malignancy, inflammatory bowel disease, diverticulosis and left inguinal hernia containing sigmoid colon is present
stiff rectal catheters are used
colonography performed only short interval following optical colonoscopy in which biopsies were performed
manual insufflation of gas
Advantages
Virtual colonoscopy has several advantages over optical colonoscopy:
less invasive procedure, therefore complication rate lower
takes less time
can visualize colon beyond the obstruction or narrowing
detects extracolonic pathology
Disadvantages
residual fecal material can give rise to wrong interpretation
biopsy specimen cannot be taken at the time of the procedure
exposure to ionizing radiation





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.