
Quadrigeminal cistern lipomas make up approximately 25% of intracranial lipomas and are located within the quadrigeminal cistern. They may be associated with hypoplasia of the inferior colliculus or agenesis of the corpus callosum.
For a general discussion please refer to the article on intracranial lipomas.
On this page:
Clinical presentation
They are usually asymptomatic and are usually found incidentally. Rarely do they cause mass effect resulting in seizures or hydrocephalus 7. Due to their location, If symptomatic, patients usually present with diplopia, disturbances in behavior due to brainstem compression and signs of hydrocephalus 9.
Radiographic features
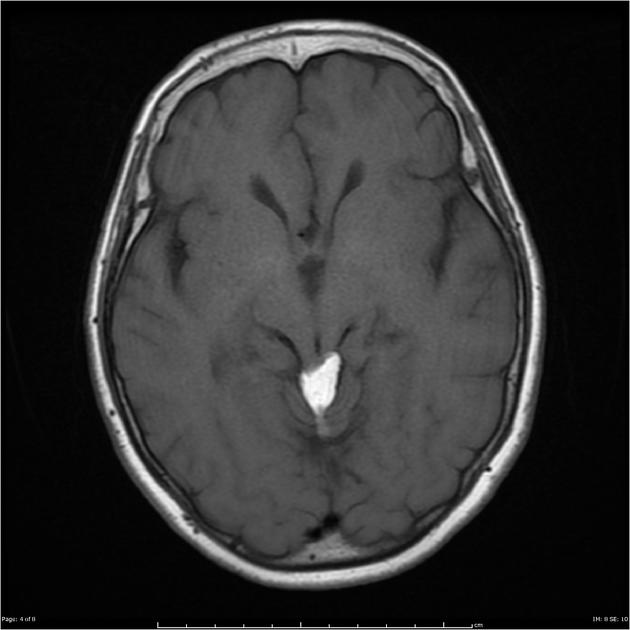
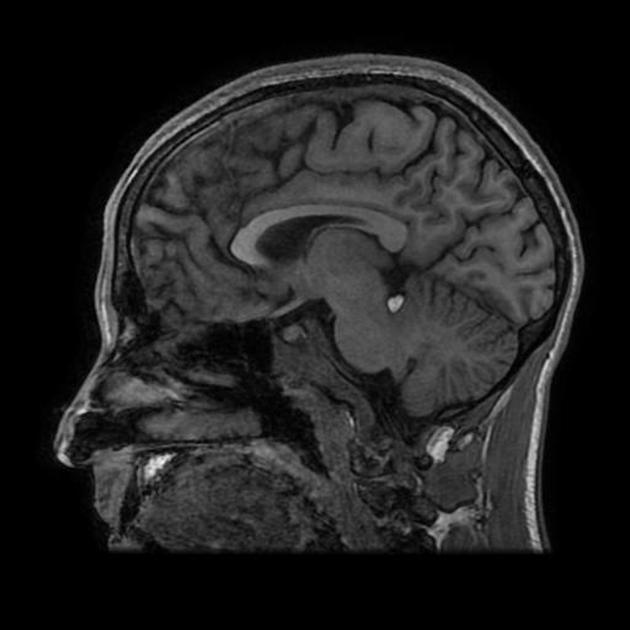
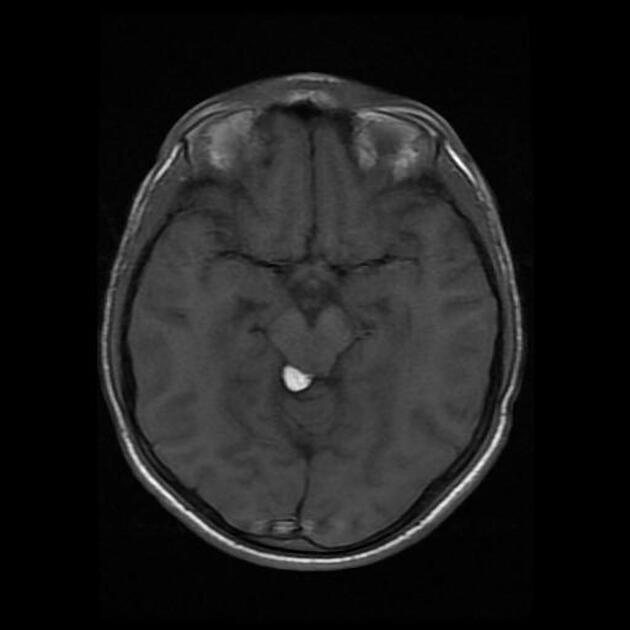
CT and MRI findings are characteristic for a fat-containing mass or lesion, however located in the quadrigeminal cistern.
CT
CT demonstrates a lobulated, non-enhancing fat attenuating (often (HU = − 50 to − 100) mass in the quadrigeminal cistern. Peripheral calcification can be present in some cases.
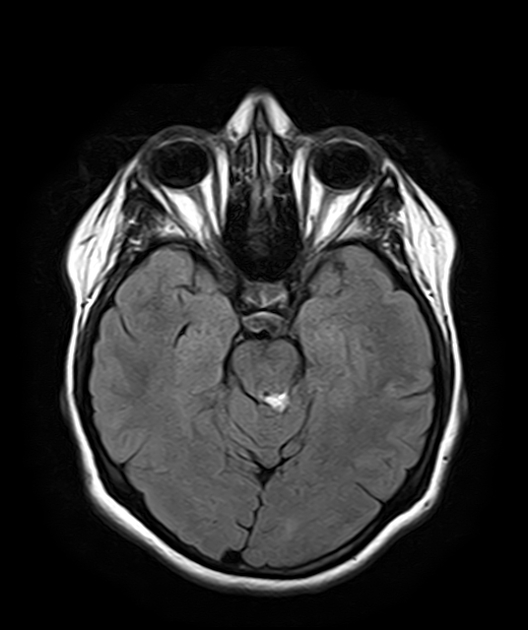
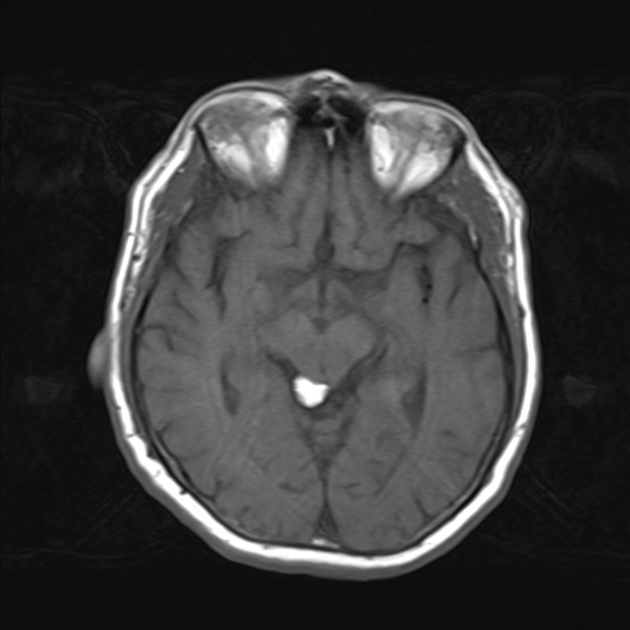
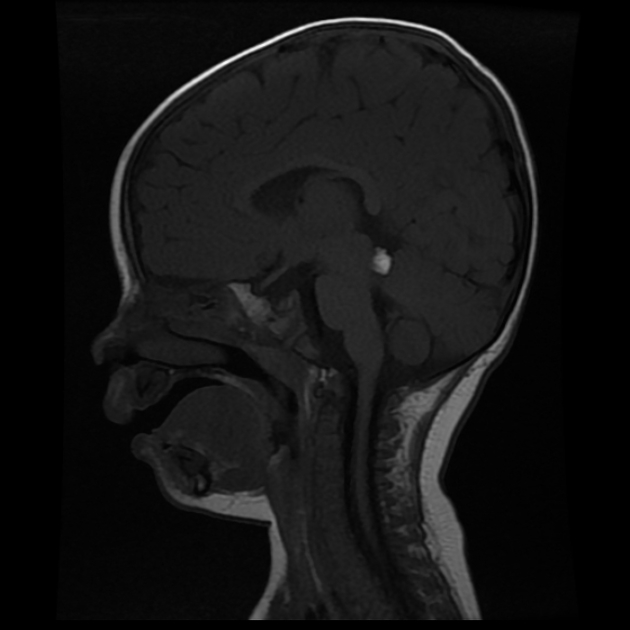
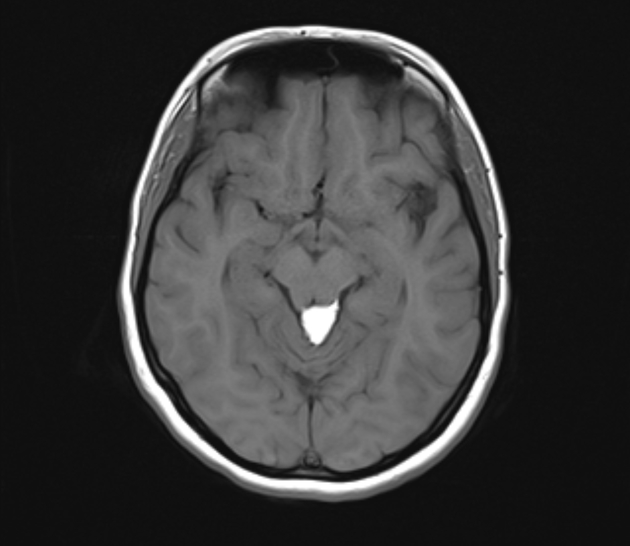
MRI
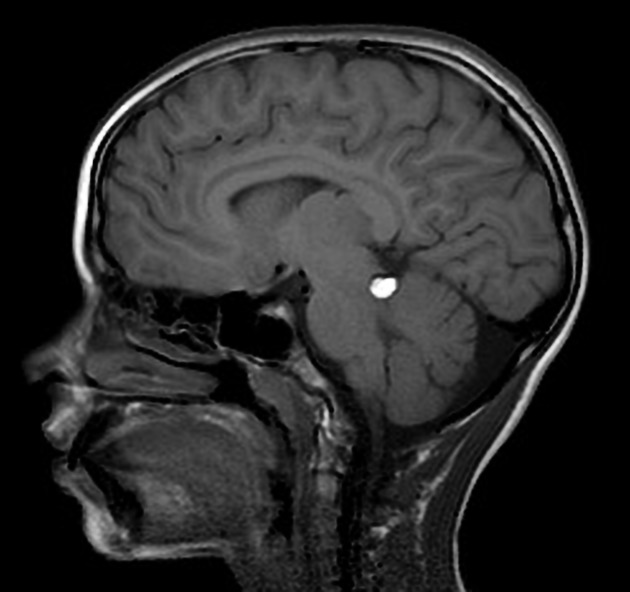
MRI reveals signal characteristic of fat:
T1: high signal intensity
T2: high signal intensity
T1 C+ (Gd): no enhancement
fat saturated sequences: low signal intensity
SWI: can produce blooming due to susceptibility artifact 8
Treatment and prognosis
Lipomas, in general, are mostly asymptomatic. Asymptomatic lesions often do not require treatment. If there is mass effect causing seizures or hydrocephalus, then surgical management can be considered 4,6,7. Endoscopic approach is a less invasive surgical option as it limits exposure and cerebellar retraction 9.
Differential diagnosis
Differentials specific to its location (quadrigeminal plate) include tectal plate glioma or mass, tectal plate cyst, arachnoid cyst, dermoid cyst and epidermoid cyst 7.










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.