
Aspergillomas are mass-like fungus balls (mycetomas) typically composed of Aspergillus fumigatus and are a non-invasive form of pulmonary aspergillosis. They usually fall under the subgroup chronic pulmonary aspergillosis.
On this page:
Epidemiology
Aspergillomas occur in patients with normal immune status but structurally abnormal lungs, with pre-existing cavitation. Demographics will, therefore, match those with various addditional underlying conditions, such as 2:
pulmonary tuberculosis: most common, accounting for 25-80% of cases depending on the prevalence of tuberculosis in the population 2,3
bronchiectasis from any cause
-
other pulmonary cavities
Clinical presentation
Most aspergillomas are asymptomatic. Occasionally due to surrounding reactive vascular granulation tissue, hemoptysis may be present. Occasionally, erosion into a bronchial artery may lead to life-threatening hemoptysis 1.
Pathology
An aspergilloma is a type of mycetoma, which is described by the 2024 Fleischner glossary as a mass-like collection of fungal hyphae, mixed with mucous, fibrin, and cellular debris, within a pre-existing cavity 6. The walls of the cavity consist of vascular granulation tissue 1,2.
Location
Aspergillomas typically occur in the cavities of post-primary pulmonary tuberculosis. Therefore, they are most frequently found in the posterior segments of the upper lobes and the superior segments of the lower lobes.
Radiographic features
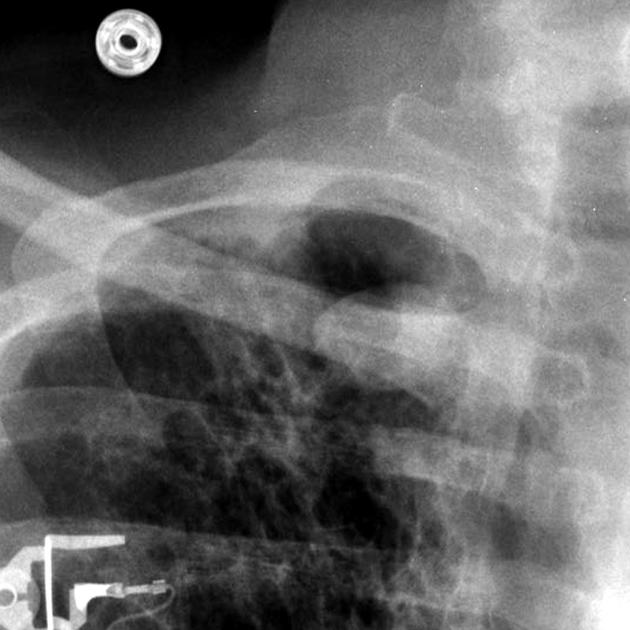
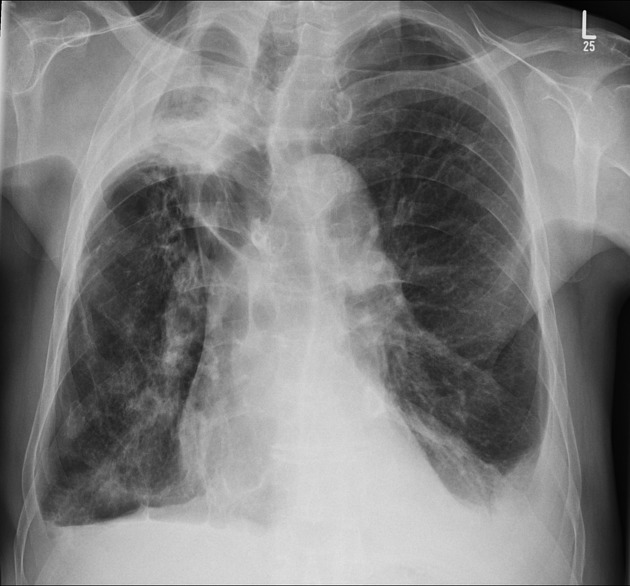
Plain radiograph
An aspergilloma can be seen as a mass within a cavity. The mass is typically spherical or ovoid. The air around the aspergilloma takes a crescentic shape, termed the air crescent sign (previously known as the Monod sign). On different patient positioning, the mass can be shown to be mobile.
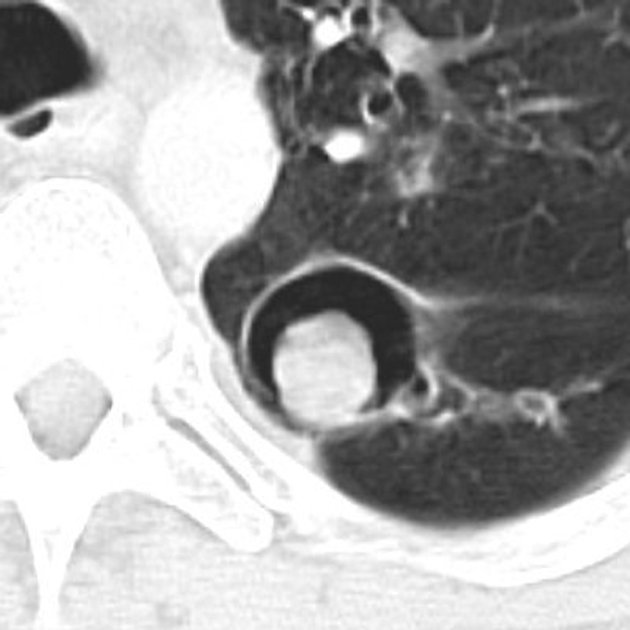
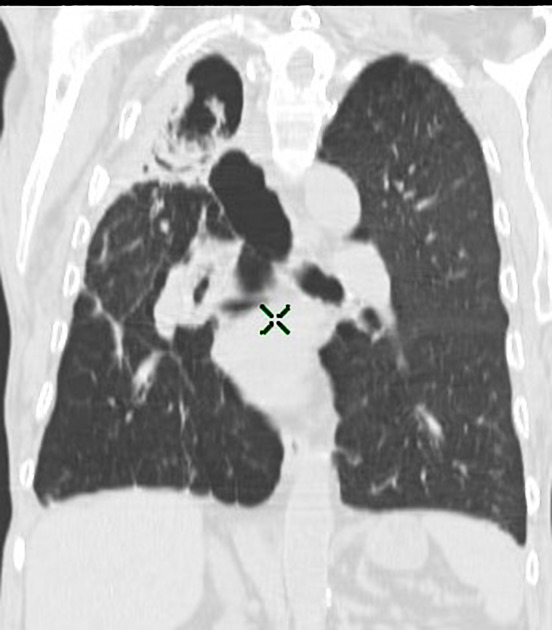
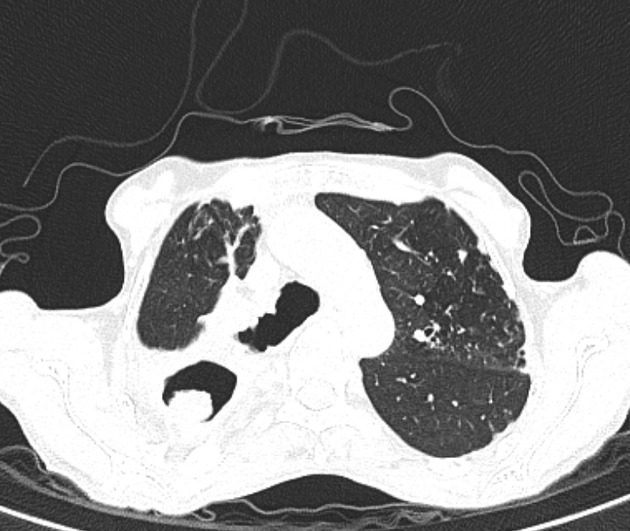
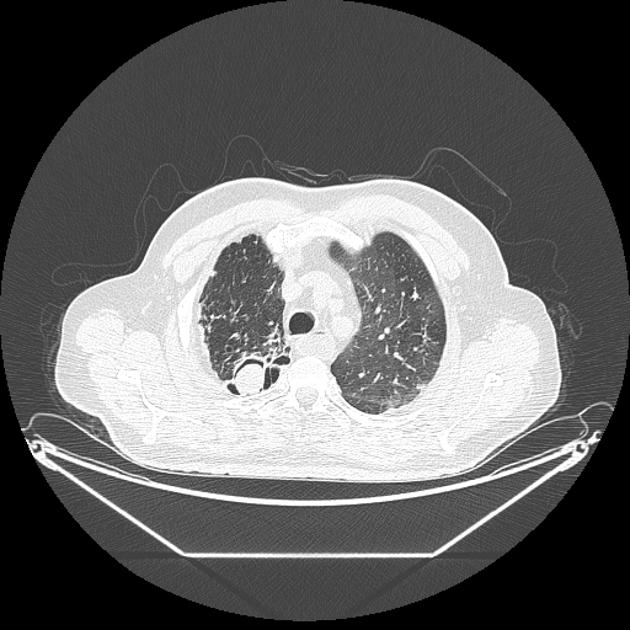
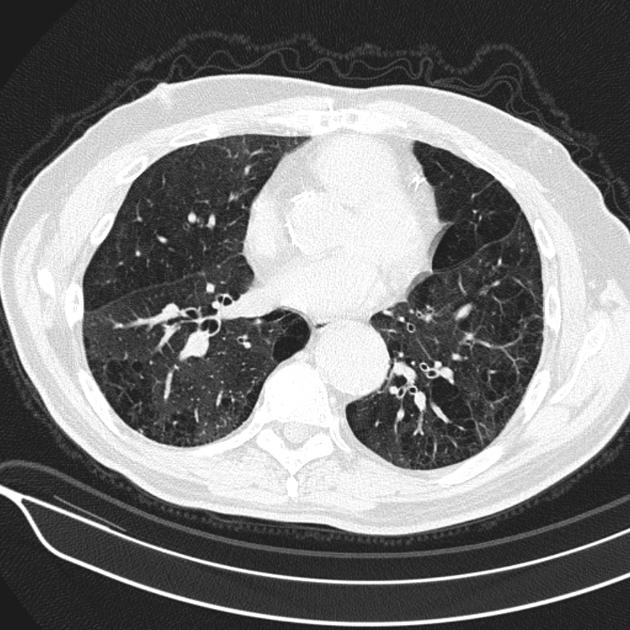
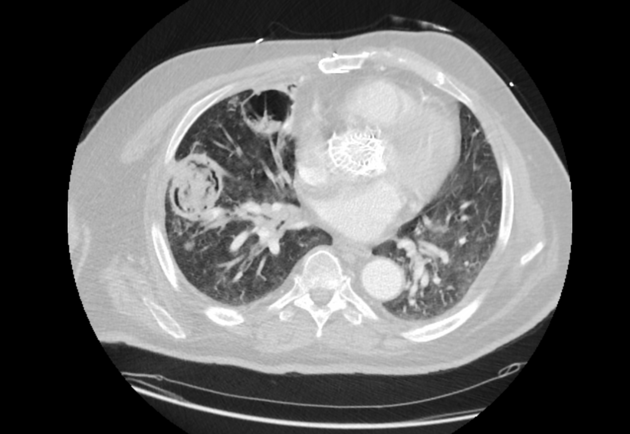
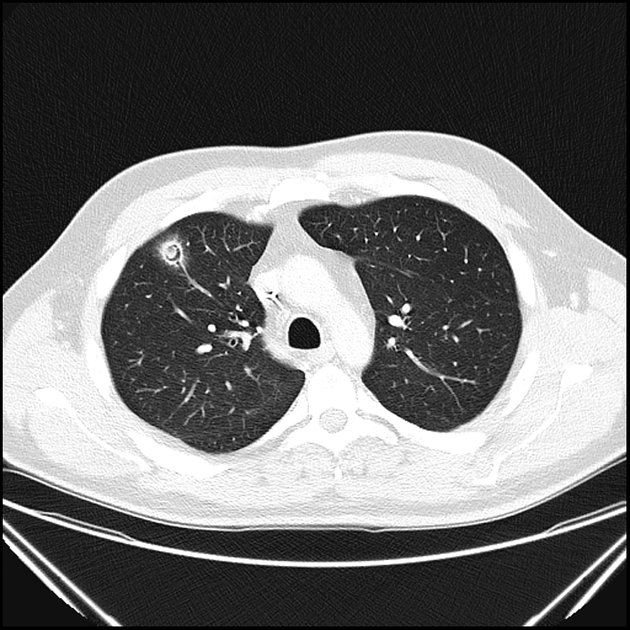
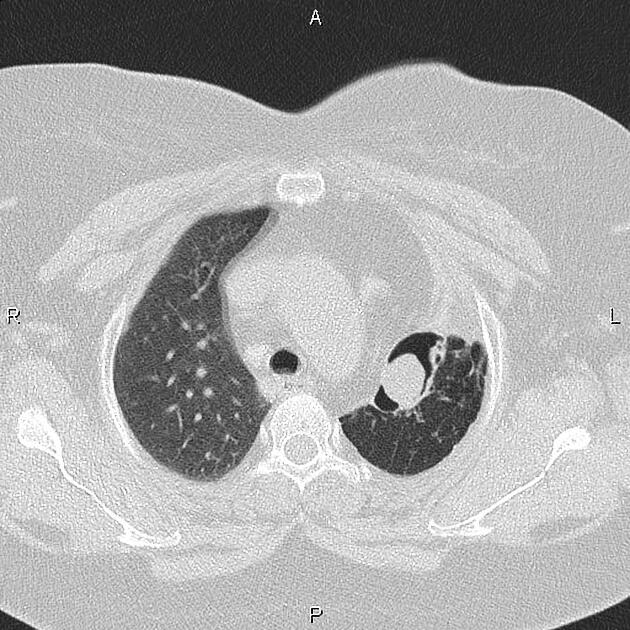
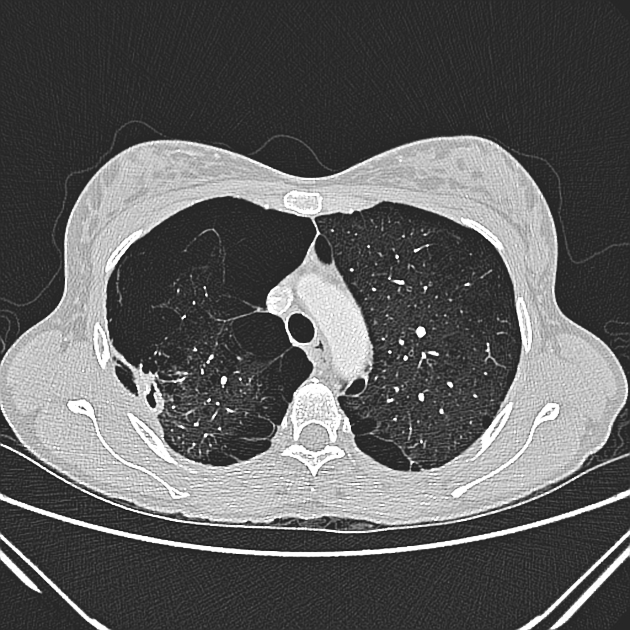
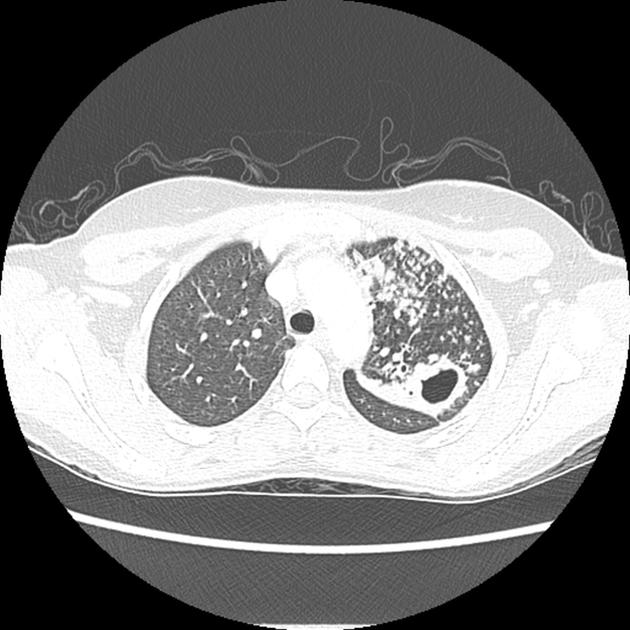
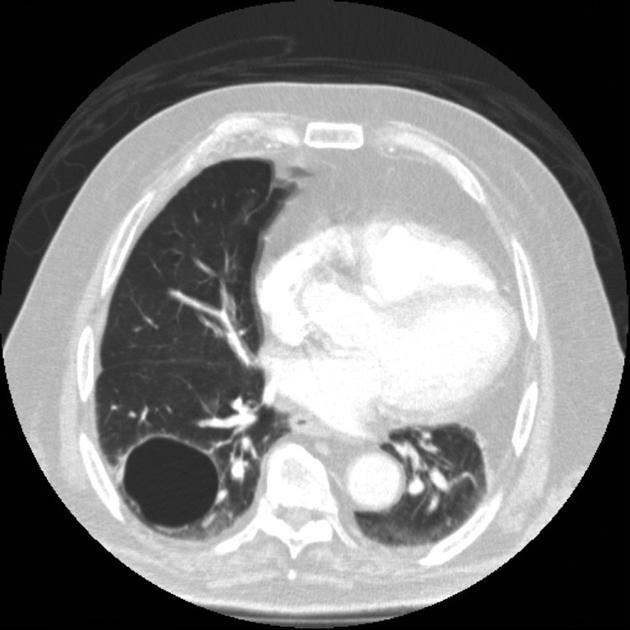
CT
CT better demonstrates the plain radiographic findings of a rounded mass within a cavity. The air crescent sign around the mass is usually present and mobility of the mass can be demonstrated between prone and supine positioning. On occasion the mass may entirely fill the cavity, thus taking on the shape of the cavity, obliterating the surrounding air crescent and no longer being mobile 2. The mass is soft tissue attenuation but calcification is not uncommon.
Due to the inflammation and vascular granulation tissue formation, the bronchial arteries supplying the wall can be enlarged 2. The adjacent pleura may well be thickened.
Treatment and prognosis
An asymptomatic aspergilloma does not necessarily require treatment, and the cavity is essentially isolated from any systemic administration of antifungal 3.
In the setting of brisk hemoptysis, angiography may be performed on an emergency basis and selective bronchial artery embolization can be life-saving. Failing this, or in cases of repeated hemoptysis, surgical excision with a lobectomy remains the gold standard 3.
The mortality rate varies widely, but in more series, it is observed to be low, even in cases where surgery is required 3.
Differential diagnosis
When classical in appearance, there is little difference. If the mass fills the cavity completely then the differential is that of a solitary pulmonary nodule.










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.