
Chordoid meningiomas are uncommon histological variants of meningiomas, and due to their predilection for rapid growth and local recurrence are designated as grade 2 tumors under the (5th Edition) WHO classification of CNS tumors.
Chordoid tumors are encountered in a very wide age range (possibly somewhat younger than other meningiomas 3), in a wide range of locations within the intracranial cavity and have clinical presentations indistinguishable from other meningiomas 1,2. These are therefore discussed in the main meningioma article.
An association with Castleman disease was part of the original description but is only uncommonly encountered 3-5.
On this page:
Pathology
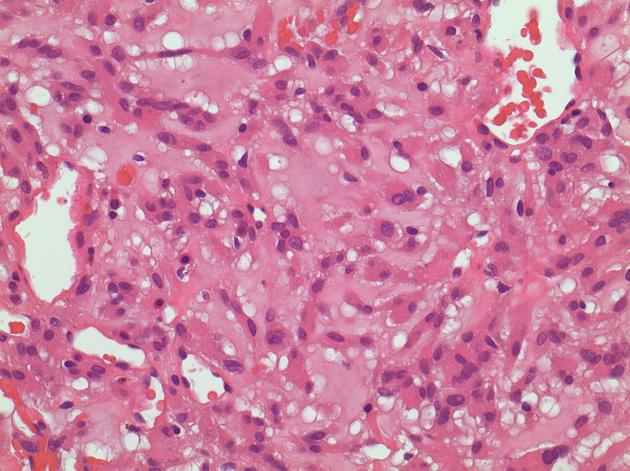
Chordoid meningiomas have characteristic histological appearances, which contribute to their distinctive diffusion characteristics on imaging (see below).
The epithelioid tumor cells demonstrate cytoplasmic vacuolization and are embedded in a mucoid matrix which has abundant hyaluronic acid and chondroitin sulfate 1,2.
The mitotic index of these tumors has been variably reported (0.4-11.4%) and it is likely that this is not the underlying cause of higher reported recurrence rate 3.
Chordoid tumors are usually vimentin EMA positive, and GFAP negative 5.
Radiographic features
MRI
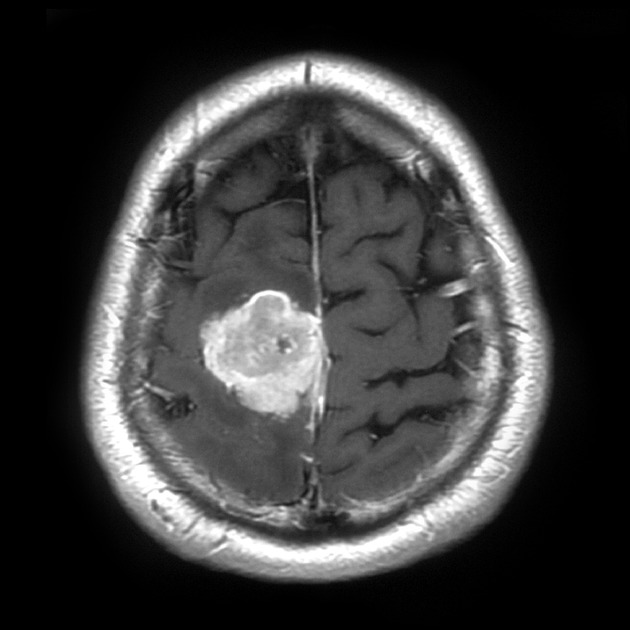
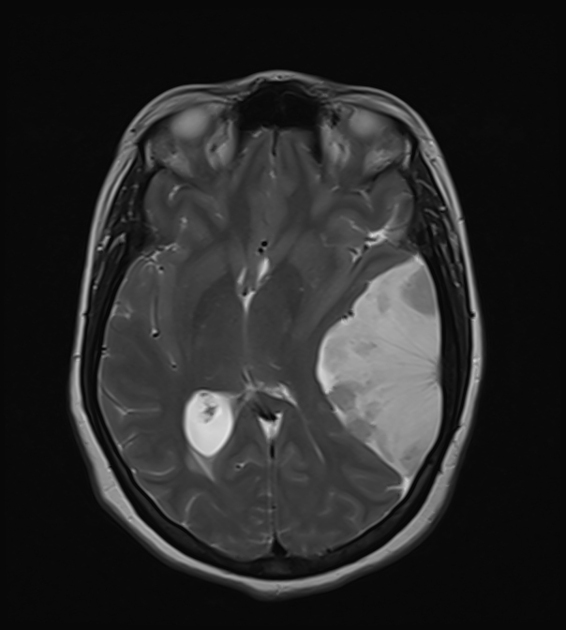
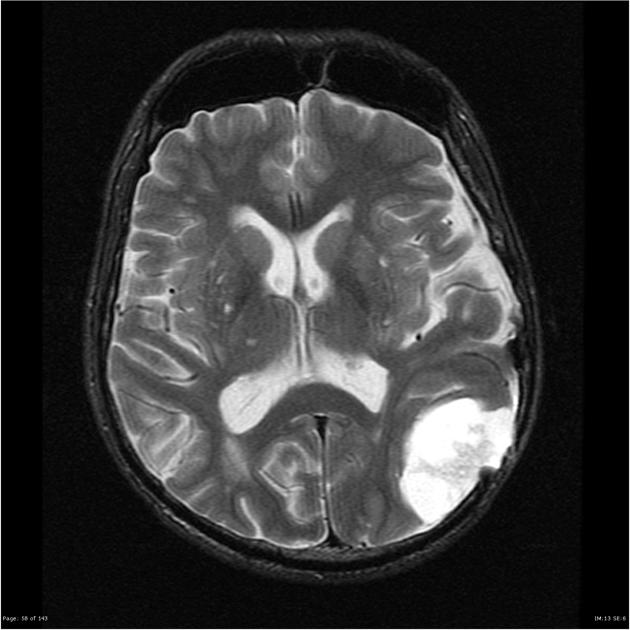
T1 and T2 signal characteristics are generally similar to other meningiomas, and no morphological features are particularly helpful in distinguishing chordoid meningiomas from other variants 1. Generally, they are probably more heterogeneous and perhaps more likely to involve adjacent bone, however, limited numbers in reported series make this difficult to assess 1,2.
-
T1
typically isointense to grey matter (same as typical grade 1 meningiomas)
-
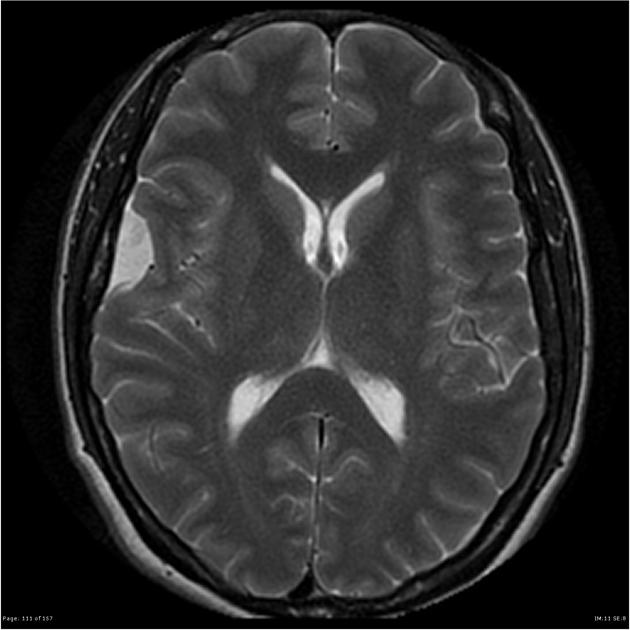
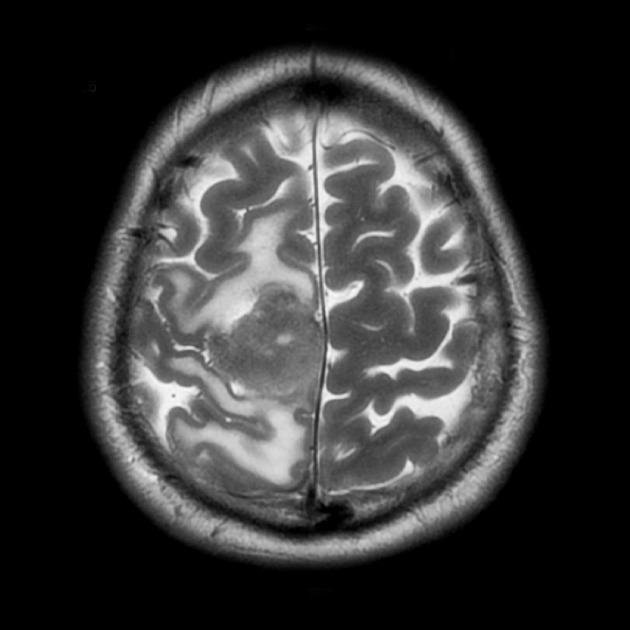
T2
typically mildly hyperintense to grey matter (grade 1 tumors are typically isointense)
peritumoral edema is variable (absent to pronounced)
-
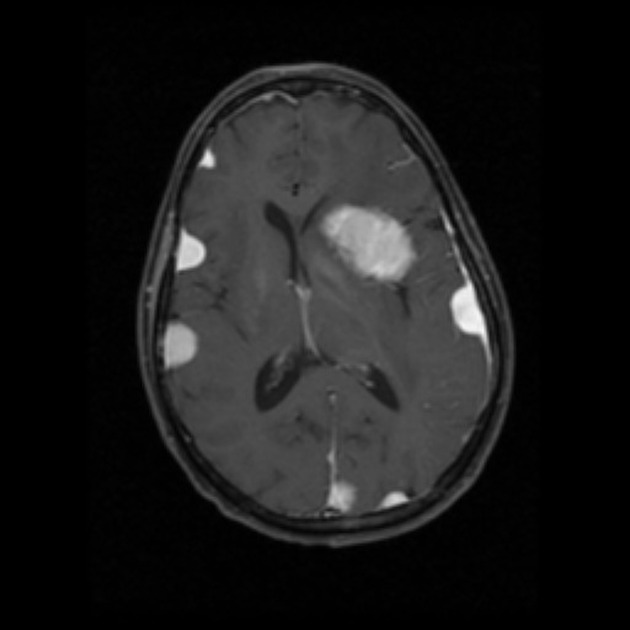
T1 C+
most are vividly enhancing
occasional areas of non-enhancement due to necrosis are identified 1
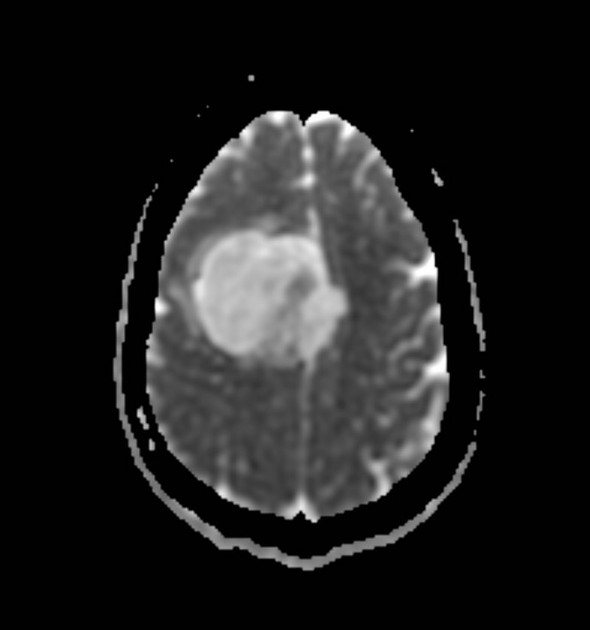
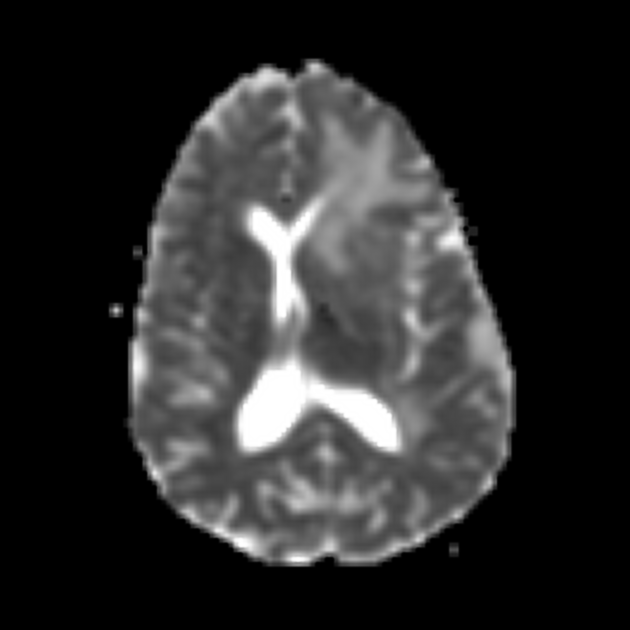
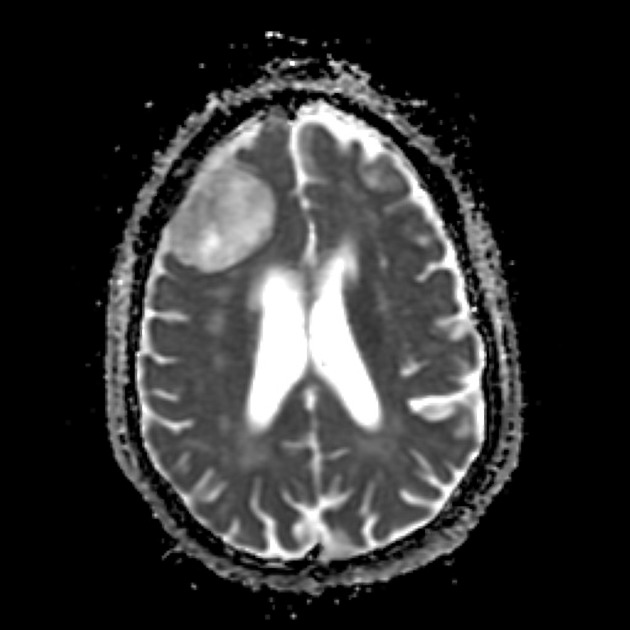
The most helpful MRI feature in distinguishing a chordoid meningiomas from other histological variants are their diffusion characteristics. They typically have facilitated diffusion with a mean ADC value of 1620 +/- 330 x 10-6 mm2/s according to one study 1. In contrast, WHO grade 1 meningiomas, non-chordoid grade 2 tumors and grade 3 tumors all have more pronounced diffusion restriction, similar or lower to brain parenchyma (around 800 x 10-6 mm2/s).
Treatment and prognosis
Chordoid meningiomas are treated with surgical excision and if complete resection is accomplished then a cure is possible. In subtotal resection (Simpson grade 4) or in cases of recurrence, radiotherapy is also often used 5.
They are, however, considered WHO grade 2 tumors on account of a higher rate of local recurrence (up to 42%) 3.
History and etymology
Chordoid meningiomas were first described in 1980 (single case report in a 15-year old) 6 and subsequently named 1988 4.
Differential diagnosis
In addition to all other histological variants of meningiomas (especially microcystic subtype), chordoid meningiomas need to be distinguished from other extra-axial tumors with an abundant extracellular matrix. Therefore the differential includes:
-
typically demonstrate brighter T2 signal
less facilitated diffusion 1
-
typically arising in the midline from the clivus
almost invariably associated with bony destruction
-
typically arising from the central base of the skull, near the petroclival synchondrosis
may have chondroid ossification (rings and arcs)
myxoid soft-tissue tumors





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.