

Congestive cardiac failure
Updates to Article Attributes
Congestive cardiac failure (CCF), also known as congestive heart failure (CHF) or simply heart failure, refers to the clinical syndrome caused by inherited or acquired abnormalities of heart structure and function, causing a constellation of symptoms and signs that lead to decreased quality and quantity of life.
Epidemiology
CCF is common, affecting 2% of all adults in developed nations, and up to 10% of adults over 65 years old 1. The condition is thought to affect up to 20 million people worldwide 1.
Clinical presentation
Clinical presentation varies considerably depending on the severity and aetiology of CCF 1,2. Traditionally, symptoms can be clustered into either being attributed toventricular dysfunction orand right ventricular dysfunction, although in realityrespectively, most patients will have manifestations from both clusters 1,2.
- left-predominant symptoms and signs
-
exertional dyspnoea and fatigue1,2-
orthopnoea: dyspnoea in the recumbent positionfatigue,may use multiple pillows at night1,2 -
paroxysmal nocturnal dyspnoea: dyspnoea that awakens the patient from sleep, usually only after 1-2 hours, and may have a chronic nocturnal cough and cardiac asthma1,2- subjective discomfort or difficulty breathing
-
bendopnoea: dyspnoea while bending forward3
-
angina1,2 -
syncope and cerebral dysfunction1,2 -
cyanosis1,2 -
other organ dysfunction1,2 -
addedabnormal auscultatory heart sounds 1,2-
S3 ‘ventricular gallop’ (occurs after S2an audible "S3" may be appreciated during early diastole and/or an "S4" in late diastole-
the former may originate from taut mitral subvalvular structures secondary to ventricular dilation, and
is due to blood slushing around in a large dilated ventricle)1,2 -
S4 ‘atrial gallop’ (occurs before S1 and is due to blood enteringtheventricle during atrial systole hitting the stiff hypertrophiedlatter from decreased ventricularwall1,2
-
the former may originate from taut mitral subvalvular structures secondary to ventricular dilation, and
-
- pulsus alternans 1,2
-
- right-predominant symptoms and signs
-
nocturia1,2- nocturia
-
dependent, pitting oedema
- commonly bipedal or sacral
-
sacral and scrotal oedema, especially if bed bound1,2 -
peripheral (ankle) oedema1,2 -
ascites
1,2 -
hepatomegaly
, may have a tender edge and gastrointestinal symptoms1,2 -
raisedjugular venouspressure1,2
The severity of clinical presentation and functional status of a patient is often classified according to the New York Heart Association (NYHA), which assigns a grade between I and IV dependent on symptoms and on how limited the physical activity has become 1,2:
- NYHA I: no symptoms during normal physical activity, no limitation
- NYHA II: symptoms during ordinary physical activity, slight limitation
- NYHA III: symptoms during less than ordinary physical activity, marked limitation (patients generally only comfortable at rest)
- NYHA IV: symptoms even when at rest, severe limitation
Pathology
Classification
Patients with end-stage CCF may have Cheyne-Stokes respiration, hypotension, tachycardia, featuresIn the presence ofvalvulopathiescardiac cachexia1,2.Depending ontheunderlying aetiology, additional clinical features may also be present1,2.PathologyIt may be precipitated by intrinsicpresence of diastolic dysfunction and/or structural cardiacor extrinsic factorsabnormalities (e.g.It may also be acute (acute decompensated cardiac failureleft atrial dilation, left ventricular hypertrophy)or chronic (chronic congestive cardiac failure)1,2. Up to 40-50% ofhave diastolic heart failure with preserved left ventricular function4.Classification and aetiologyTherearenumerous ways of classifying CCF, the mostcommonlyutilised being a functional classification that is based on cardiac output and ejection fraction1,2. In this classification, there are often overlapping aetiologies and patients can move from one classification to the other over time1,2.Another key classifier of heart failure isgrouped by left ventricular ejection fraction (LVEF) as follows:-
heart failure with a reduced ejection fraction
(LVEF(HFrEF), derived by dividing the left ventricular stroke volume by end-diastolic volume. While heart failure is not defined by the degree-
those with an LVEF of
left ventricular impairment, the classification is crucial for treatment decisions;<40% - current therapy is based primarily on large clinical trials only enrolling those with ejection fractions below 40%15
.In patients with reduced systolic function the LVEF is lower and the intracardiac volumes higher. A cutoff LVEF of <40% in the presence of a suggestive clinical syndrome defines HFrEF. Intermediate ejection fractions (between 40-50%) are typically grouped in the HFrEF phenotype.Clinical heart failure with an ejection fraction >50% defines the HFpEF syndrome; in these patients with heart failure symptoms in whom reductions in ejection fraction do not occur, there is generally a prominent increase in the left ventricular wall thickness and progressive dilation of the left atrium. low-output heart failure
-
those with an LVEF of
- heart failure with
reduceda preserved ejection fraction(HFrEF(HFpEF), previously termed 'systolic- an LVEF equal to or greater than 50%
- heart failure
'with a midrange ejection fraction (HFmrEF)- those falling between the abovementioned cutoffs (40-49%)
Etiology
While significant overlap exists, etiological associations may correspond to the phenotypes delineated by LVEF as follows:
-
associated with a decreased left ventricular ejection fraction
- ischaemic dilated cardiomyopathy 1,2
- non-ischaemic dilated cardiomyopathy
- idiopathic
- infectious
-
toxic (e.g.
idiopathicalcoholism,alcohol)
-
tachycardia-mediated cardiomyopathy
, -
Chagas disease
, -
Duchenne muscular dystrophy
, -
peripartum
/postpartumcardiomyopathy, -
hypothyroidism
, cocaine use, infection, etc.)1,2
- regurgitant valve disease
- left-to-right shunts
-
associated with a preserved left ventricular ejection fraction
- chronic hypertension 1,2
-
obstructive valve disease (e.g. in the setting ofvalvulopathies-
aortic valve stenosis
)1,2 -
regurgitant valve disease (e.g. in the setting ofaortic valve regurgitation)1,2 -
left-to-right shunts (e.g.atrial septal defect,ventricular septal defect,patent ductus arteriosus,Gerbode defect,atrioventricular septal defect, etc.)1,2
-
aortic valve stenosis
-
heart failure with preserved ejection fraction (HFpEF), previously termed 'diastolicinfiltrative diseases -
radiation-induced heart
failure'- disease
-
hypertrophic cardiomyopathy
(e.g.-
hypertrophic obstructive cardiomyopathy
, -
Yamaguchi syndrome
, chronichypertension, obstructive valve disease, left-to-right shunts,
-
hypertrophic obstructive cardiomyopathy
-
athlete's heart
, -
Danon disease
, etc.)1,2 -
restrictive cardiomyopathy
(e.g.cardiac amyloidosis,cardiac sarcoidosis,endomyocardial fibrosis,haemochromatosis,radiation-induced heart disease, etc.) - constrictive pericarditis 1,2
-
-
-
A somewhat distinct entity is that of high-output heart failure in which a primary decrease in systemic vascular resistance triggers a neurohormonal cascade akin to that observed with a decreased cardiac output. Etiologies of this syndrome include:
- morbid obesity 1,2
- systemic arteriovenous shunts
(e.g. - chronic lung disease 1,2
- sepsis 1,2
- myeloproliferative neoplasm 1,2
- anaemia 1,2
- hyperthyroidism 1,2
- wet beriberi 1,2
- carcinoid syndrome 1,2
Radiographic features
Plain radiograph
The accuracy of interpreting chest radiographs regarding congestive cardiac failure was only around 70% according to one study 5.
With left-sided congestive cardiac failure, the features are that of pulmonary oedema which includes 1,2,4-8:
- pulmonary venous congestion
- cephalisation of pulmonary veins
- pulmonary interstitial oedema
- pulmonary alveolar oedema
- cardiomegaly (may or may not be present depending on aetiology)
- pleural effusion
Ultrasound: echocardiography
Echocardiography is the most common imaging modality used to evaluate patients with CCF 1,2. It is able to provide a semi-quantitative assessment of left ventricular size and function and determine the presence of valvular or wall abnormalities 1,2. Variables near ubiquitouslyinduring a complete transthoracic echocardiography exam include:
-
the systolicleft ventricular functionof the left ventricle- the surrogate measure ejection fraction is
the most populara common method
- the surrogate measure ejection fraction is
-
thediastolic functionof the left ventricleperturbations are often appreciable before the systolic function is affected
- structure of the left ventricle
- wall thickness and left ventricular end-diastolic internal diameter may yield a derived mass, the basis of diagnosing remodeling and hypertrophy
CT
CT chest may demonstrate the same features as the plain radiograph but in greater detail and clarity 6,7,9. Furthermore, electrocardiograph-gated CT and cardiac CT angiography may provide estimates of cardiac function and detailed visualisation of various cardiac structures 9. Mediastinal lymph node enlargement may be present in some cases 13,14.
MRI
Cardiac MRI (CMR) is able to provide highly accurate ejection fraction estimates and determine the presence of any structural abnormalities and is considered by many to be the gold standard imaging modality 2,9-11. Patterns of late gadolinium enhancement can distinguish between many aetiologies of CCF, although this is beyond the scope of this general article on CCFmay be useful in delineating an etiology 10,11.
Treatment and prognosis
Treatment involves a multidisciplinary team and incorporates lifestyle, allied health, pharmacological, and even surgical therapies, often specific to the underlying aetiology 1,2. An in-depth review of the treatment of CCF is beyond the scope of this article, however, generalGeneral principles include:
- treatment of comorbidities and complications
(e.g. obesity, hypertension, depression, etc.)1,2 - lifestyle interventions
: education, cessation of smoking and alcohol consumption, increase in isotonic exercise, improve diet, daily home weights1,2 - pharmacotherapy
:-
mortality benefit:depending on clinical context, examples include angiotensin-converting-enzyme inhibitors, angiotensin II receptor blockers,combination angiotensin receptor-neprilysin inhibitors (sacubitril/valsartan), betabeta-blockers(only carvedilol, bisoprolol, metoprolol succinate, nebivolol), spironolactone, nitrates and digoxin11,2,12-
these medications only have a benefit in patients with HFrEF, there are no medications with a mortality benefit in HFpEF (as of December 2017)1,2
-
-
symptomatic benefit with no mortality benefitinvasive/surgical management may include:other diuretics, nitrates, digoxin, hydralazine1,2
-
-
surgery: considerimplantable cardioverter-defibrillators, - cardiac resynchronisation therapy
, -
ventricular assist devices,
and even -
cardiac transplant
, depending on the severity and aetiology1,2
Despite advances in management in recent decades, prognosis remains poor with 30-40% of patients dying within 1 year, and up to 70% dying within 5 years 1.
Complications
- acute decompensated heart failure
and - acute pulmonary oedema
- passive hepatic congestion
- cardiorenal syndrome
- dysrhythmias
See also
-<p><strong>Congestive cardiac failure (CCF)</strong>, also known as <strong>congestive heart failure (CHF) </strong>or simply<strong> heart failure</strong>, refers to the clinical syndrome caused by inherited or acquired abnormalities of heart structure and function, causing a constellation of symptoms and signs that lead to decreased quality and quantity of life.</p><h4>Epidemiology</h4><p>CCF is common, affecting 2% of all adults in developed nations, and up to 10% of adults over 65 years old <sup>1</sup>. The condition is thought to affect up to 20 million people worldwide <sup>1</sup>.</p><h4>Clinical presentation</h4><p>Clinical presentation varies considerably depending on the severity and aetiology of CCF <sup>1,2</sup>. Traditionally, symptoms can be clustered into either being attributed to left ventricular dysfunction or right ventricular dysfunction, although in reality, most patients will have manifestations from both clusters <sup>1,2</sup>.</p><ul>-<li>left-predominant symptoms and signs<ul>-<li>exertional dyspnoea and fatigue <sup>1,2</sup><ul>-<li>orthopnoea: dyspnoea in the recumbent position, may use multiple pillows at night <sup>1,2</sup>- +<p><strong>Congestive cardiac failure (CCF)</strong>, also known as <strong>congestive heart failure (CHF) </strong>or simply<strong> heart failure</strong>, refers to the clinical syndrome caused by inherited or acquired abnormalities of heart structure and function, causing a constellation of symptoms and signs that lead to decreased quality and quantity of life.</p><h4>Epidemiology</h4><p>CCF is common, affecting 2% of all adults in developed nations, and up to 10% of adults over 65 years old <sup>1</sup>. The condition is thought to affect up to 20 million people worldwide <sup>1</sup>.</p><h4>Clinical presentation</h4><p>Clinical features traditionally associated with left and right ventricular dysfunction, respectively, may include;</p><ul>
- +<li>left-predominant symptoms and signs <sup>1,2</sup><ul>
- +<li>fatigue, syncope</li>
- +<li>dyspnoea<ul><li>subjective discomfort or difficulty breathing</li></ul>
-<li>paroxysmal nocturnal dyspnoea: dyspnoea that awakens the patient from sleep, usually only after 1-2 hours, and may have a chronic nocturnal cough and cardiac asthma <sup>1,2</sup>- +<li>chest pain</li>
- +<li>abnormal auscultatory heart sounds <sup>1,2</sup><ul><li>an audible "S3" may be appreciated during early diastole and/or an "S4" in late diastole<ul><li>the former may originate from taut mitral subvalvular structures secondary to ventricular dilation, and the latter from decreased ventricular compliance</li></ul>
- +</li></ul>
-<li>bendopnoea: dyspnoea while bending forward <sup>3</sup>- +<li>pulsus alternans <sup>1,2</sup>
-<li>angina <sup>1,2</sup>-</li>-<li>syncope and cerebral dysfunction <sup>1,2</sup>-</li>-<li>cyanosis <sup>1,2</sup>-</li>-<li>other organ dysfunction <sup>1,2</sup>-</li>-<li>added heart sounds <sup>1,2</sup><ul>-<li>S3 ‘ventricular gallop’ (occurs after S2 and is due to blood slushing around in a large dilated ventricle) <sup>1,2</sup>-</li>-<li>S4 ‘atrial gallop’ (occurs before S1 and is due to blood entering the ventricle during atrial systole hitting the stiff hypertrophied ventricular wall <sup>1,2</sup>- +<li>right-predominant symptoms and signs <sup>1,2</sup><ul>
- +<li>nocturia </li>
- +<li>dependent, pitting oedema<ul><li>commonly bipedal or sacral</li></ul>
- +<li><a href="/articles/ascites">ascites</a></li>
- +<li>
- +<a href="/articles/hepatomegaly">hepatomegaly</a> </li>
- +<li>jugular venous distension </li>
-<li>pulsus alternans <sup>1,2</sup>- +</ul><p>The severity of clinical presentation and functional status of a patient is often classified according to the New York Heart Association (NYHA), which assigns a grade between I and IV dependent on symptoms and on how limited the physical activity has become <sup>1,2</sup>:</p><ul>
- +<li>
- +<strong>NYHA I</strong>: no symptoms during normal physical activity, no limitation</li>
- +<li>
- +<strong>NYHA II</strong>: symptoms during ordinary physical activity, slight limitation</li>
- +<li>
- +<strong>NYHA III</strong>: symptoms during less than ordinary physical activity, marked limitation (patients generally only comfortable at rest)</li>
- +<li>
- +<strong>NYHA IV</strong>: symptoms even when at rest, severe limitation</li>
- +</ul><h4>Pathology</h4><h5>Classification</h5><p>In the presence of consistent symptoms and clinical signs, elevated natiuretic peptides, and the presence of diastolic dysfunction and/or structural cardiac abnormalities (e.g. left atrial dilation, left ventricular hypertrophy), patients are commonly grouped by left ventricular <a title="Left ventricular ejection fraction (echocardiography)" href="/articles/left-ventricular-ejection-fraction-echocardiography">ejection fraction</a> (LVEF) as follows:</p><ul>
- +<li>heart failure with a reduced ejection fraction (HFrEF)<ul>
- +<li>those with an LVEF of <40%</li>
- +<li>current therapy is based primarily on large clinical trials only enrolling those with ejection fractions below 40% <sup>15</sup>
-<li>right-predominant symptoms and signs<ul>-<li>nocturia <sup>1,2</sup>- +<li>heart failure with a preserved ejection fraction (HFpEF)<ul><li>an LVEF equal to or greater than 50%</li></ul>
-<li>sacral and scrotal oedema, especially if bed bound <sup>1,2</sup>- +<li>heart failure with a midrange ejection fraction (HFmrEF)<ul><li>those falling between the abovementioned cutoffs (40-49%)</li></ul>
-<li>peripheral (ankle) oedema <sup>1,2</sup>- +</ul><h5>Etiology</h5><p>While significant overlap exists, etiological associations may correspond to the phenotypes delineated by LVEF as follows:</p><ul>
- +<li>associated with a decreased left ventricular ejection fraction <ul>
- +<li>ischaemic <a href="/articles/dilated-cardiomyopathy">dilated cardiomyopathy</a> <sup>1,2</sup>
-<li>-<a href="/articles/ascites">ascites</a> <sup>1,2</sup>- +<li>non-ischaemic <a href="/articles/dilated-cardiomyopathy">dilated cardiomyopathy</a> <ul>
- +<li><a href="/articles/idiopathic-dilated-cardiomyopathy">idiopathic</a></li>
- +<li><a title="infectious cardiomyopathy" href="/articles/infectious-cardiomyopathy">infectious</a></li>
- +<li>toxic (e.g. sympathomimetics, alcohol)</li>
- +</ul>
- +<li><a href="/articles/tachycardia-induced-cardiomyopathy">tachycardia-mediated cardiomyopathy</a></li>
- +<li><a href="/articles/chagas-disease">Chagas disease</a></li>
- +<li><a href="/articles/duchenne-muscular-dystrophy">Duchenne muscular dystrophy</a></li>
- +<li><a href="/articles/peripartumpostpartum-cardiomyopathy-1">peripartum cardiomyopathy</a></li>
-<a href="/articles/hepatomegaly">hepatomegaly</a>, may have a tender edge and gastrointestinal symptoms <sup>1,2</sup>-</li>-<li>raised jugular venous pressure <sup>1,2</sup>- +<a href="/articles/hypothyroidism">hypothyroidism</a><sup>1,2</sup>
-</ul><p>The severity of clinical presentation and functional status of a patient is often classified according to the New York Heart Association (NYHA), which assigns a grade between I and IV dependent on symptoms and on how limited the physical activity has become <sup>1,2</sup>:</p><ul>-<li>-<strong>NYHA I</strong>: no symptoms during normal physical activity, no limitation</li>- +<li>regurgitant valve disease<ul>
-<strong>NYHA II</strong>: symptoms during ordinary physical activity, slight limitation</li>-<li>-<strong>NYHA III</strong>: symptoms during less than ordinary physical activity, marked limitation (patients generally only comfortable at rest)</li>- +<a href="/articles/aortic-valve-regurgitation">aortic valve regurgitation</a> <sup>1,2</sup>
- +</li>
- +<li><a title="mitral valve regurgitation" href="/articles/mitral-valve-regurgitation">mitral valve regurgitation</a></li>
- +</ul>
- +</li>
- +<li>left-to-right shunts<ul>
- +<li><a href="/articles/atrial-septal-defect-2">atrial septal defect</a></li>
- +<li><a href="/articles/ventricular-septal-defect-1">ventricular septal defect</a></li>
- +<li><a href="/articles/patent-ductus-arteriosus">patent ductus arteriosus</a></li>
- +<li><a href="/articles/gerbode-defect">Gerbode defect</a></li>
-<strong>NYHA IV</strong>: symptoms even when at rest, severe limitation</li>-</ul><p>Patients with end-stage CCF may have Cheyne-Stokes respiration, hypotension, tachycardia, features of <a href="/articles/valvular-heart-disease">valvulopathies</a>, and cardiac cachexia <sup>1,2</sup>. </p><p>Depending on the underlying aetiology, additional clinical features may also be present <sup>1,2</sup>. </p><h4>Pathology</h4><p>It may be precipitated by intrinsic cardiac or extrinsic factors. It may also be acute (acute decompensated cardiac failure) or chronic (chronic congestive cardiac failure) <sup>1,2</sup>. Up to 40-50% of patients have diastolic heart failure with preserved left ventricular function<sup> 4</sup>. </p><h5>Classification and aetiology</h5><p>There are numerous ways of classifying CCF, the most commonly utilised being a functional classification that is based on cardiac output and ejection fraction <sup>1,2</sup>. In this classification, there are often overlapping aetiologies and patients can move from one classification to the other over time <sup>1,2</sup>.</p><p>Another key classifier of heart failure is by left ventricular ejection fraction (LVEF), derived by dividing the left ventricular stroke volume by end-diastolic volume. While heart failure is not defined by the degree of left ventricular impairment, the classification is crucial for treatment decisions; current therapy is based primarily on large clinical trials only enrolling those with ejection fractions below 40% <sup>15</sup>.</p><p>In patients with reduced systolic function the LVEF is lower and the intracardiac volumes higher. A cutoff LVEF of <40% in the presence of a suggestive clinical syndrome defines HFrEF. Intermediate ejection fractions (between 40-50%) are typically grouped in the HFrEF phenotype.</p><p>Clinical heart failure with an ejection fraction >50% defines the HFpEF syndrome; in these patients with heart failure symptoms in whom reductions in ejection fraction do not occur, there is generally a prominent increase in the left ventricular wall thickness and progressive dilation of the left atrium.</p><ul>-<li>low-output heart failure<ul>-<li>heart failure with reduced ejection fraction (HFrEF), previously termed 'systolic heart failure'<ul>-<li>ischaemic <a href="/articles/dilated-cardiomyopathy">dilated cardiomyopathy</a> <sup>1,2</sup>- +<a href="/articles/atrioventricular-septal-defect">atrioventricular septal defect</a> <sup>1,2</sup>
-<li>non-ischaemic <a href="/articles/dilated-cardiomyopathy">dilated cardiomyopathy</a> (e.g. <a href="/articles/idiopathic-dilated-cardiomyopathy">idiopathic</a>, alcoholism, <a href="/articles/tachycardia-induced-cardiomyopathy">tachycardia-mediated cardiomyopathy</a>, <a href="/articles/chagas-disease">Chagas disease</a>, <a href="/articles/duchenne-muscular-dystrophy">Duchenne muscular dystrophy</a>, <a href="/articles/peripartumpostpartum-cardiomyopathy-1">peripartum/postpartum cardiomyopathy</a>, <a href="/articles/hypothyroidism">hypothyroidism</a>, cocaine use, infection, etc.) <sup>1,2</sup>- +</ul>
- +<li>associated with a preserved left ventricular ejection fraction<ul>
-<li>obstructive valve disease (e.g. in the setting of <a href="/articles/aortic-valve-stenosis">aortic valve stenosis</a>) <sup>1,2</sup>- +<li>valvulopathies<ul><li>
- +<a href="/articles/aortic-valve-stenosis">aortic valve stenosis</a> <sup>1,2</sup>
- +</li></ul>
- +</li>
- +</ul>
-<li>regurgitant valve disease (e.g. in the setting of <a href="/articles/aortic-valve-regurgitation">aortic valve regurgitation</a>) <sup>1,2</sup>- +<li>infiltrative diseases<ul>
- +<li><a href="/articles/cardiac-amyloidosis">cardiac amyloidosis</a></li>
- +<li><a href="/articles/sarcoidosis-cardiac-manifestations-1">cardiac sarcoidosis</a></li>
- +<li><a href="/articles/endomyocardial-fibrosis">endomyocardial fibrosis</a></li>
- +<li><a href="/articles/haemochromatosis-cardiac-manifestations-1">haemochromatosis</a></li>
- +</ul>
-<li>left-to-right shunts (e.g. <a href="/articles/atrial-septal-defect-2">atrial septal defect</a>, <a href="/articles/ventricular-septal-defect-1">ventricular septal defect</a>, <a href="/articles/patent-ductus-arteriosus">patent ductus arteriosus</a>, <a href="/articles/gerbode-defect">Gerbode defect</a>, <a href="/articles/atrioventricular-septal-defect">atrioventricular septal defect</a>, etc.) <sup>1,2</sup>- +<li>
- +<a href="/articles/haemochromatosis-cardiac-manifestations-1"></a><a href="/articles/radiation-induced-heart-disease">radiation-induced heart disease</a>
- +<li>
- +<a href="/articles/hypertrophic-cardiomyopathy">hypertrophic cardiomyopathy</a><ul>
- +<li><a href="/articles/hypertrophic-cardiomyopathy">hypertrophic obstructive cardiomyopathy</a></li>
- +<li><a href="/articles/apical-hypertrophic-cardiomyopathy">Yamaguchi syndrome</a></li>
-<li>heart failure with preserved ejection fraction (HFpEF), previously termed 'diastolic heart failure'<ul>- +<li><a href="/articles/athlete-s-heart">athlete's heart</a></li>
-<a href="/articles/hypertrophic-cardiomyopathy">hypertrophic cardiomyopathy</a> (e.g. <a href="/articles/hypertrophic-cardiomyopathy">hypertrophic obstructive cardiomyopathy</a>, <a href="/articles/apical-hypertrophic-cardiomyopathy">Yamaguchi syndrome</a>, chronic <a href="/articles/hypertension">hypertension</a>, obstructive valve disease, left-to-right shunts, <a href="/articles/athlete-s-heart">athlete's heart</a>, <a href="/articles/danon-disease">Danon disease</a>, etc.) <sup>1,2</sup>- +<a href="/articles/danon-disease">Danon disease</a> <sup>1,2</sup>
-<a href="/articles/restrictive-cardiomyopathy">restrictive cardiomyopathy</a> (e.g. <a href="/articles/cardiac-amyloidosis">cardiac amyloidosis</a>, <a href="/articles/sarcoidosis-cardiac-manifestations-1">cardiac sarcoidosis</a>, <a href="/articles/endomyocardial-fibrosis">endomyocardial fibrosis</a>, <a href="/articles/haemochromatosis-cardiac-manifestations-1">haemochromatosis</a>, <a href="/articles/radiation-induced-heart-disease">radiation-induced heart disease</a>, etc.) <sup>1,2</sup>- +<a href="/articles/restrictive-cardiomyopathy">restrictive cardiomyopathy</a> <sup>1,2</sup>
-</ul>-</li>-</ul>- +</ul><p>A somewhat distinct entity is that of <a href="/articles/high-output-cardiac-failure">high-output heart failure</a> in which a primary decrease in <a title="systemic vascular resistance" href="/articles/systemic-vascular-resistance">systemic vascular resistance</a> triggers a neurohormonal cascade akin to that observed with a decreased cardiac output. Etiologies of this syndrome include:</p><ul>
- +<li>morbid <a href="/articles/obesity">obesity</a> <sup>1,2</sup>
- +<li>systemic arteriovenous shunts<ul>
- +<li><a href="/articles/hereditary-haemorrhagic-telangiectasia">hereditary haemorrhagic telangiectasia</a></li>
- +<li><a href="/articles/hepatopulmonary-syndrome">hepatopulmonary syndrome</a></li>
-<a href="/articles/high-output-cardiac-failure">high-output heart failure</a><ul>-<li>morbid <a href="/articles/obesity">obesity</a> <sup>1,2</sup>- +<a href="/articles/haemodialysis-arteriovenous-fistula">haemodialysis fistula</a> <sup>1,2</sup>
-<li>systemic arteriovenous shunts (e.g. <a href="/articles/hereditary-haemorrhagic-telangiectasia">hereditary haemorrhagic telangiectasia</a>, <a href="/articles/hepatopulmonary-syndrome">hepatopulmonary syndrome</a>, <a href="/articles/haemodialysis-arteriovenous-fistula">haemodialysis fistula</a>) <sup>1,2</sup>- +</ul>
-</ul>-</li>-<li><a href="/articles/pulmonary-venous-congestion">pulmonary venous congestion</a></li>- +<li><a title="Pulmonary edema" href="/articles/pulmonary-oedema">pulmonary venous congestion</a></li>
-</ul><h5>Ultrasound: echocardiography</h5><p>Echocardiography is the most common imaging modality used to evaluate patients with CCF <sup>1,2</sup>. It is able to provide a semi-quantitative assessment of left ventricular size and function and determine the presence of valvular or wall abnormalities <sup>1,2</sup>. Variables near ubiquitously assessed in a complete <a href="/articles/transthoracic-echocardiography-views">transthoracic echocardiography</a> exam include</p><ul>-<li>the systolic function of the left ventricle<ul><li>the surrogate measure <a href="/articles/left-ventricular-ejection-fraction-echocardiography">ejection fraction</a> is the most popular method</li></ul>-</li>-<li>the <a href="/articles/diastolic-dysfunction-point-of-care-ultrasound">diastolic</a> function of the left ventricle<ul><li>perturbations are often appreciable before the systolic function is affected</li></ul>-</li>- +</ul><h5>Ultrasound</h5><p>Echocardiography is the most common imaging modality used to evaluate patients with CCF <sup>1,2</sup>. Some features assessed during a complete <a href="/articles/transthoracic-echocardiography-views">transthoracic echocardiography</a> exam include:</p><ul>
- +<li>left ventricular function<ul>
- +<li>the surrogate measure <a href="/articles/left-ventricular-ejection-fraction-echocardiography">ejection fraction</a> is a common method to estimate global systolic function</li>
- +<li>
- +<a href="/articles/diastolic-dysfunction-point-of-care-ultrasound">diastolic</a> function may also be assessed, involving spectral Doppler as well as 2D measurements</li>
-<li>the right ventricular structure and <a href="/articles/right-ventricular-dysfunction">function</a><ul><li>more technically challenging, <a href="/articles/right-heart-strain">RV strain</a> lacks parameters to assess to nearly the same degree as the left ventricle</li></ul>-</li>-</ul><h5>CT</h5><p>CT chest may demonstrate the same features as the plain radiograph but in greater detail and clarity <sup>6,7,9</sup>. Furthermore, electrocardiograph-gated CT and cardiac CT angiography may provide estimates of cardiac function and detailed visualisation of various cardiac structures <sup>9</sup>. <a href="/articles/mediastinal-lymph-node-enlargement">Mediastinal lymph node enlargement</a> may be present in some cases <sup>13,14</sup>.</p><h5>MRI</h5><p>Cardiac MRI (CMR) is able to provide highly accurate ejection fraction estimates and determine the presence of any structural abnormalities and is considered by many to be the gold standard imaging modality <sup>2,9-11</sup>. Patterns of late gadolinium enhancement can distinguish between many aetiologies of CCF, although this is beyond the scope of this general article on CCF <sup>10,11</sup>.</p><h4>Treatment and prognosis</h4><p>Treatment involves a multidisciplinary team and incorporates lifestyle, allied health, pharmacological, and even surgical therapies, often specific to the underlying aetiology <sup>1,2</sup>. An in-depth review of the treatment of CCF is beyond the scope of this article, however, general principles include:</p><ul>-<li>treatment of comorbidities and complications (e.g. obesity, hypertension, depression, etc.) <sup>1,2</sup>- +</ul>
-<li>lifestyle interventions: education, cessation of smoking and alcohol consumption, increase in isotonic exercise, improve diet, daily home weights <sup>1,2</sup>- +<li>valvular anatomy and function</li>
- +<li>right ventricular structure and <a href="/articles/right-ventricular-dysfunction">function</a>
-<li>pharmacotherapy: <ul>-<li>mortality benefit: angiotensin-converting-enzyme inhibitors, angiotensin II receptor blockers, combination angiotensin receptor-neprilysin inhibitors (sacubitril/valsartan), beta-blockers (only carvedilol, bisoprolol, metoprolol succinate, nebivolol), spironolactone <sup>1,2,12</sup><ul><li>these medications only have a benefit in patients with HFrEF, there are no medications with a mortality benefit in HFpEF (as of December 2017) <sup>1,2</sup>- +<li>pericardial space</li>
- +</ul><h5>CT</h5><p>CT chest may demonstrate the same features as the plain radiograph but in greater detail and clarity <sup>6,7,9</sup>. Furthermore, electrocardiograph-gated CT and cardiac CT angiography may provide estimates of cardiac function and detailed visualisation of various cardiac structures <sup>9</sup>. <a href="/articles/mediastinal-lymph-node-enlargement">Mediastinal lymph node enlargement</a> may be present in some cases <sup>13,14</sup>.</p><h5>MRI</h5><p><a title="Cardiac MRI" href="/articles/cardiac-mri">Cardiac MRI</a> (CMR) is able to provide highly accurate ejection fraction estimates and determine the presence of any structural abnormalities and is considered by many to be the gold standard imaging modality <sup>2,9-11</sup>. Patterns of late gadolinium enhancement may be useful in delineating an etiology <sup>10,11</sup>.</p><h4>Treatment and prognosis</h4><p>Treatment involves a multidisciplinary team and incorporates lifestyle, allied health, pharmacological, and even surgical therapies, often specific to the underlying aetiology <sup>1,2</sup>. General principles include:</p><ul>
- +<li>treatment of comorbidities and complications</li>
- +<li>lifestyle interventions</li>
- +<li>pharmacotherapy <ul><li>depending on clinical context, examples include angiotensin-converting-enzyme inhibitors, angiotensin II receptor blockers, beta-blockers, spironolactone, nitrates and digoxin<sup> 1,2,12</sup>
-<li>symptomatic benefit with no mortality benefit: other diuretics, nitrates, digoxin, hydralazine <sup>1,2</sup>-</li>- +<li>invasive/surgical management may include: <ul>
- +<li><a href="/articles/cardiac-conduction-devices">implantable cardioverter-defibrillators</a></li>
- +<li>cardiac resynchronisation therapy</li>
- +<li>
- +<a href="/articles/ventricular-assist-device">ventricular assist devices</a>,</li>
- +<li><a href="/articles/cardiac-transplant">cardiac transplant</a></li>
-<li>surgery: consider <a href="/articles/cardiac-conduction-devices">implantable cardioverter-defibrillators</a>, cardiac resynchronisation therapy, <a href="/articles/ventricular-assist-device">ventricular assist devices</a>, and even <a href="/articles/cardiac-transplant">cardiac transplant</a>, depending on the severity and aetiology <sup>1,2</sup>-</li>-<li>acute decompensated heart failure and <a href="/articles/pulmonary-oedema">acute pulmonary oedema</a>-</li>- +<li>acute decompensated heart failure</li>
- +<li><a href="/articles/pulmonary-oedema">acute pulmonary oedema</a></li>
- +<li>cardiorenal syndrome</li>
- +<li>dysrhythmias</li>
- +<li><a title="Cardiac anatomy" href="/articles/heart">cardiac anatomy</a></li>
- +<li><a title="Transthoracic echocardiography views" href="/articles/transthoracic-echocardiography-views">echocardiography</a></li>
- +<li><a title="Cardiac MRI" href="/articles/cardiac-mri">cardiac MRI</a></li>
References changed:
- 16. Ponikowski P, Voors A, Anker S et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur Heart J. 2016;37(27):2129-200. <a href="https://doi.org/10.1093/eurheartj/ehw128">doi:10.1093/eurheartj/ehw128</a> - <a href="https://www.ncbi.nlm.nih.gov/pubmed/27206819">Pubmed</a>
Tags changed:
- cardiac
- cardiology
- medicine
- emergency
- critical
Image ( destroy )
Image ( destroy )
Image ( destroy )
Image 2 X-ray (Frontal) ( update )

Image 3 X-ray (Frontal) ( update )

Image 4 X-ray (Frontal) ( update )

Image 5 MRI (cine) ( create )

Image 6 MRI (Cine SSFP (sBTFE)) ( create )

Image 7 CT (lung window) ( update )
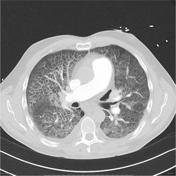
Image 8 Ultrasound (Longitudinal (left lung)) ( update )

Image 9 CT (C+ CTPA) ( create )

Image 10 X-ray (Frontal) ( create )






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.