
Choroid plexus infarct is an uncommon location of ischemic stroke that results from ischemia of the choroid plexus, supplied by the medial posterior choroidal artery, which is a branch from the posterior cerebral artery (PCA).
On this page:
Clinical presentation
Isolated choroid plexus infarction is rare and has no specific clinical features. Also, there is no known effect of choroid plexus ischemia on CSF regulation. It is usually discovered incidentally in the context of PCA infarction with clinical symptoms related to the cerebral parenchymal infarction, rather than choroid plexus infarction
Pathology
Ischemia of the choroid plexus is rare due to its rich blood supply and anastomosis of the anterior choroidal artery, a branch from the internal carotid artery, and the posterior choroidal artery, a branch from the posterior cerebral artery
The posterior choroidal artery is not a single artery (often up to 10 or 11 per hemisphere). The posterior choroidal arteries are divided into the medial posterior choroidal artery and lateral posterior choroidal artery groups. They usually arise from the P2 segment of the PCA near the thalamogeniculate perforators. The medial artery is usually the one involved in choroid plexus infarction.
The lateral ventricle choroid plexus is more susceptible to ischemia compared to that of the fourth ventricle.
Radiographic features
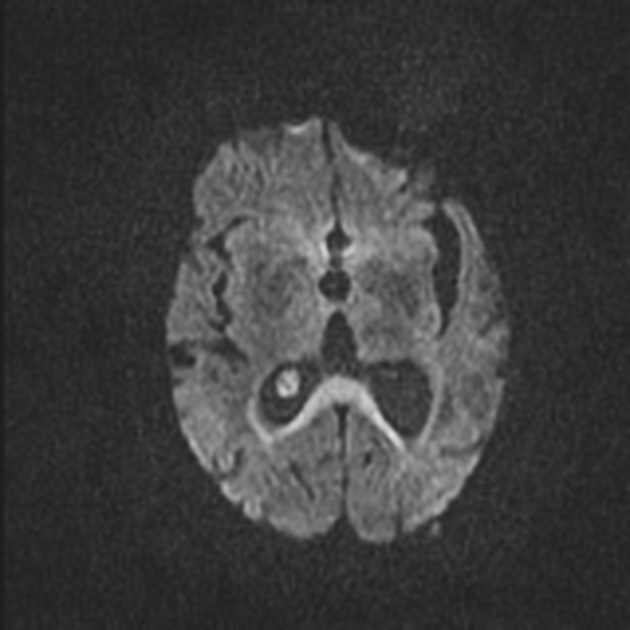
MR diffusion-weighted imaging is the main study detecting choroid plexus infarction where it appears restricted eliciting high signal in DWI and low signal in ADC. It is rare to be isolated. It is usually unilateral and associated with other infarcts along posterior cerebral artery territory especially the posterior cerebral cortex, thalamocapsular and pericallosal regions.
Angiographic studies (CT, MRI, or conventional) can demonstrate the posterior cerebral artery stenosis or occlusion.
Differential diagnosis
Considerations include
-
choroid plexus xanthogranuloma
may also appear restricted in DWI
an incidental finding with no associated other infarctions
usually bilateral
-
follow CSF in all pulse sequences with no restriction in diffusion study
an incidental finding


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.