
A breast abscess is a relatively rare but significant complication of mastitis that may occur during breastfeeding, particularly in primiparous women. The clinical context is a key to diagnosis as imaging appearances (particularly ultrasound) can mimic many other entities such as breast carcinoma.
On this page:
Epidemiology
Breast abscesses are thought to develop in 5-11% of lactating women with infectious mastitis 3. In this context they are also referred to as lactational abscesses. Note, that a neonatal breast abscess is a different entity occurring on a background of neonatal mastitis.
Clinical presentation
There is often an antecedent clinical history of mastitis. The breast usually appears hot, red, and indurated. The course may be affected by antibiotic therapy depending on when the patient is imaged.
Pathology
A breast abscess is defined as an inflammatory mass that drains purulent material either spontaneously or on incision. The predominant infectious organism is Staphylococcus aureus, often the penicillinase-producing and methicillin-resistant S. aureus 12. Other causative organisms include Staphylococcus epidermidis and Proteus mirabilis.
Peripheral breast abscesses have generally been associated with mastitis during breastfeeding, but previous reports indicate that abscesses are common among non-lactating women.
Associations
increased incidence in those with diabetes
Classification
For clinical relevance and for planning treatment breast abscesses are classified as:
puerperal abscesses: seen in primiparous mothers
non-puerperal central abscesses: commonest non-breastfeeding abscess, seen mostly in young women; especially smokers
non-puerperal peripheral abscesses: less commonly seen. Seen in older women with underlying chronic medical conditions like diabetes, rheumatoid arthritis; women taking steroids; or following recent breast intervention
Radiographic features
The clinical context is crucial to image interpretation.
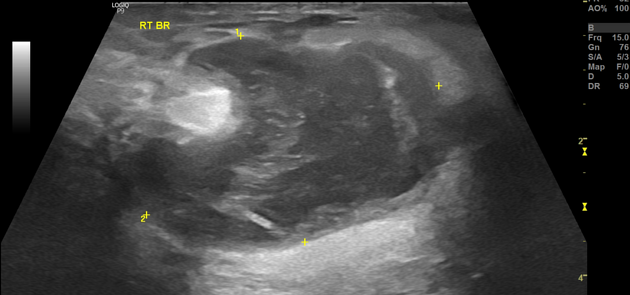
Breast ultrasound
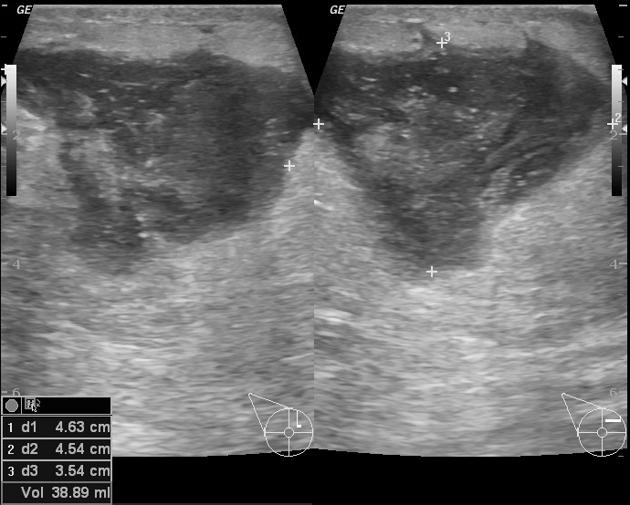
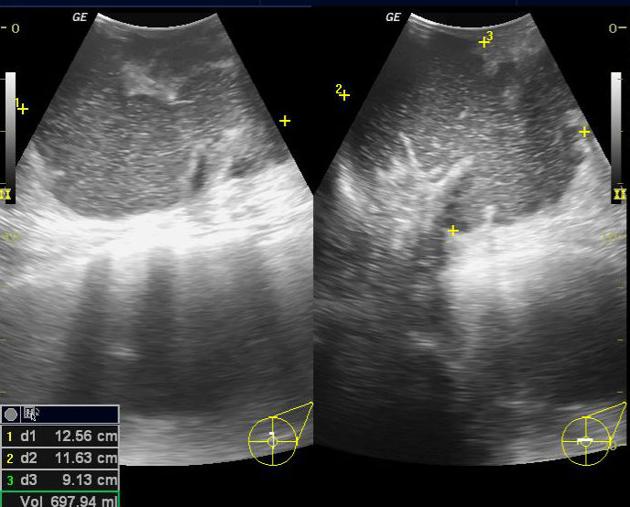
Ultrasound is considered the most useful initial imaging modality when a breast abscess is suspected. It is also the imaging method of choice to monitor progress, response to therapy and to ensure resolution. For the purpose of follow up the three dimensional measurement of the abscess and the volume of the contents should be given.
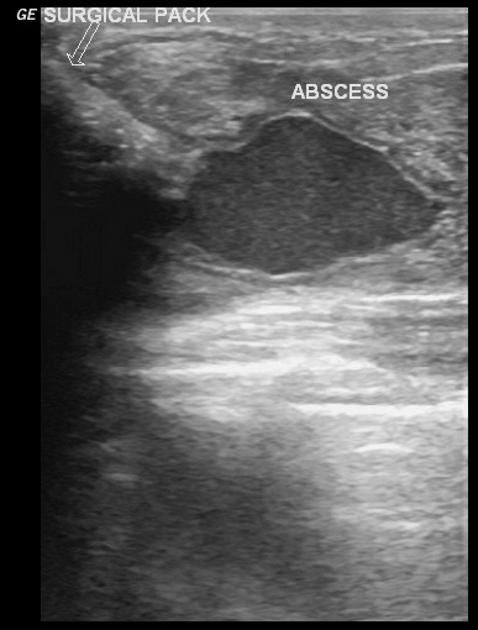
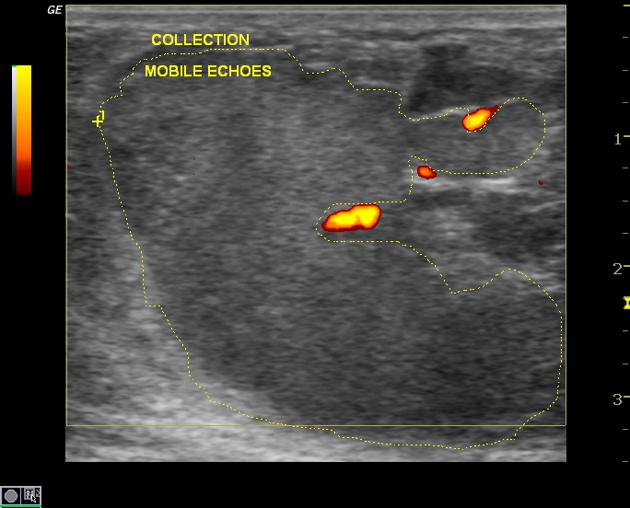
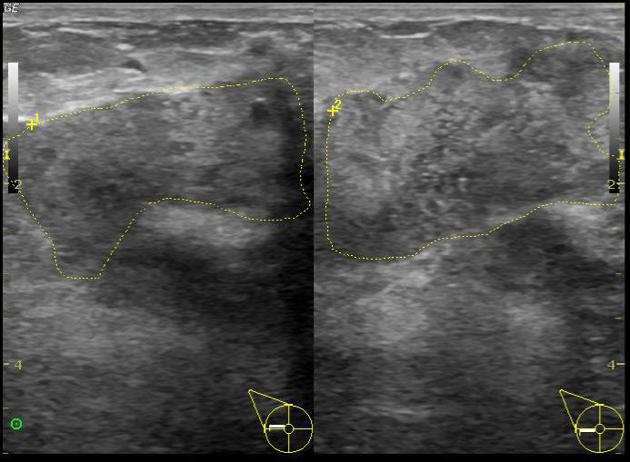
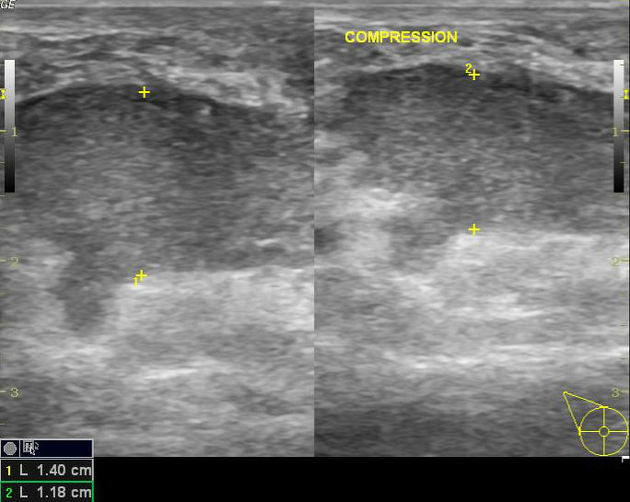
Sonographic features suggestive of a breast abscess include 11:
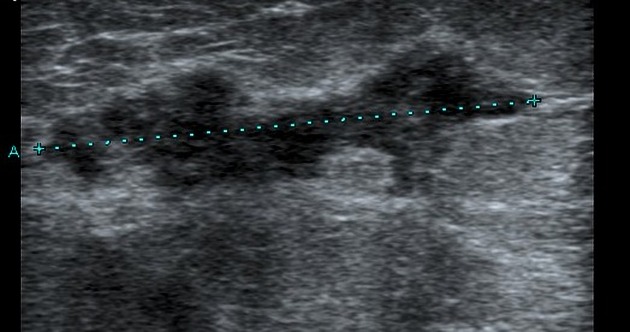
hypoechoic collection, mostly multiloculated
no vascularity within the collection
posterior acoustic enhancement due to fluid content
an echogenic, vascular rim
Mammography
Mammography is very rarely indicated or useful. Mammography is recommended to exclude the possibility of malignancy in non-puerperal abscesses, in women over 30 years and in puerperal abscesses with a prolonged clinical course. Mammographic appearances are often non specific and in the age group where breast abscesses are most often found, mammography is rarely done.
Findings which may be demonstrated are:
skin thickening
asymmetric density, mass or distortion
These findings are not specific for abscess or malignancy; however presence of suspicious microcalcifications is more specific for malignancy and a biopsy to rule out carcinoma should be carried out.
Treatment and prognosis
Antibiotic treatment combined with ultrasound-guided aspiration is the treatment of choice. Repeated aspiration may be required but is recommended over placement of percutaneous catheter due to the risk of cutaneous fistula and patient discomfort. In rare cases surgical incision and drainage may be required.
It is recommended that breastfeeding continue throughout treatment to prevent milk stasis 11.
Differential diagnosis
On ultrasound a breast abscess can easily mimic other entities such as a breast malignancy or a breast hematoma on imaging grounds alone. In practice, the most difficult differentiation is from a galactocele.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.