
Intrapulmonary lymph nodes, or pulmonary lymph nodes, are normal lymph nodes found within the lung parenchyma itself.
On this page:
Terminology
According to the 2024 Fleischner glossary, typical locations of intrapulmonary lymph nodes are described as perifissural (lying along a fissure), peripheral (close to pleura) or pleura-based (in contact with pleura other than fissural pleura). The term juxtapleural is no longer recommended 10.
The term intrapulmonary lymph node excludes mediastinal, hilar and peribronchial lymph nodes. The latter occur at bronchial bifurcations up to and including the third branch.
Epidemiology
Some publications suggest that lymph nodes may account for 24–44% of noncalcified nodules in a lung cancer screening setting 7 and may represent up to 66% of all nodules on CT scans. They are commonly seen in the mid and lower zones and can be difficult to differentiate from malignant pulmonary nodules with certainty. Nodules superior to the carina are less likely to be lymph nodes and more likely to be primary lung cancers.
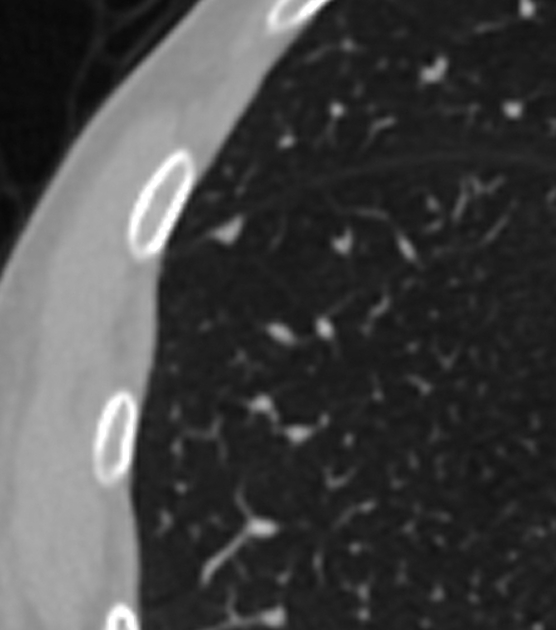
Radiographic features
CT
Thin sections and evaluation in two or three orthogonal planes underpin accurate evaluation. Intrapulmonary lymph nodes are characterized by:
location: middle and lower lobe predominant, inferior to the carina 4
pleura-based or juxtapleural (within 15 mm of a visceral pleural surface)
no effect on pleura
solid soft-tissue attenuation with no fat or calcification
sharply marginated with a smooth outline
3-15 mm diameter, usually less than 12 mm 7
elongated with an aspect ratio often >1.78
lenticular, ovoid, semicircular, triangular, trapezoidal, polygonal, faceted
lymph nodes located at the junction of interlobular septa may show a discrete thin line extending to the pleura which may be due to interlobular septum, venule or lymphatics
may grow or shrink over time
no arterial attachment
In contrast, small peripheral cancers such as adenocarcinomas may show:
arterial attachment
indistinct or irregular margin, spiculation or microlobulation
as a round nodule which may touch a pleural surface
-
signs of visceral pleural invasion 9 such as:
large area of contact for pleural attached nodules
pleural thickening
tags to multiple pleural surfaces
jellyfish sign (multiple pleural tags from the margins of a pleura-attached nodule)
85% of cancers misdiagnosed as intrapulmonary lymph nodes were in the upper lobes and this was particularly common if the features were ‘atypical’ for intrapulmonary lymph nodes 8. Upper lobe nodules should trigger extra vigilance.



 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}