
Bone islands, previously known as enostoses, are common benign sclerotic bone lesions that usually represent an incidental finding. When occurring in the head they are called osteomas. Bone islands are considered one of the skeletal “don’t touch” lesions.
On this page:
Terminology
Enostosis is not a recommended term as per the WHO classification of soft tissue and bone tumors (5th edition) 10.
Epidemiology
Bone islands are more common in males 10.
Associations
osteopoikilosis: multiple bone islands 10
See main osteoma article for further details.
Diagnosis
See main osteoma article.
Pathology
Bone islands occur in the medullary cavity, merging with trabecular bone. They may be solitary or multiple (monostotic or polyostotic). The size of a bone island is typically <1 cm, although large bone islands may occur, particularly in the pelvis, and when >2 cm in maximal dimension are called giant bone islands 4,8,10.
Location
Bone islands occur in the medullary cavity almost anywhere in the skeleton, although there is a predilection for the pelvis, long bones, spine, and ribs 10.
Radiographic features
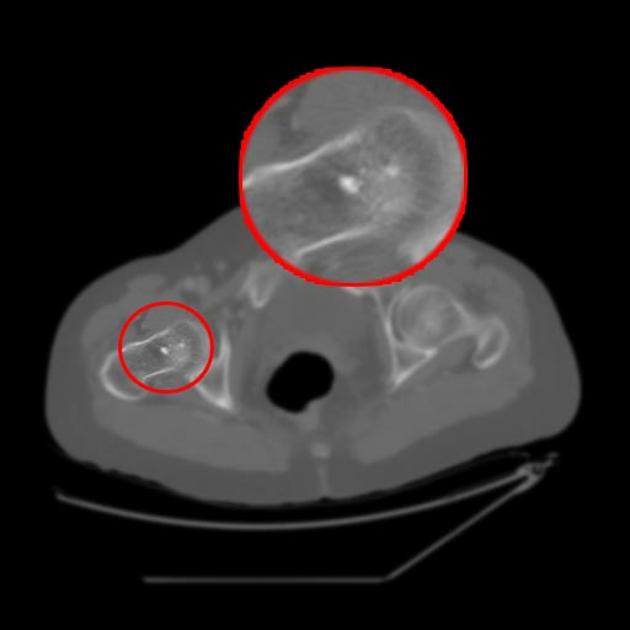
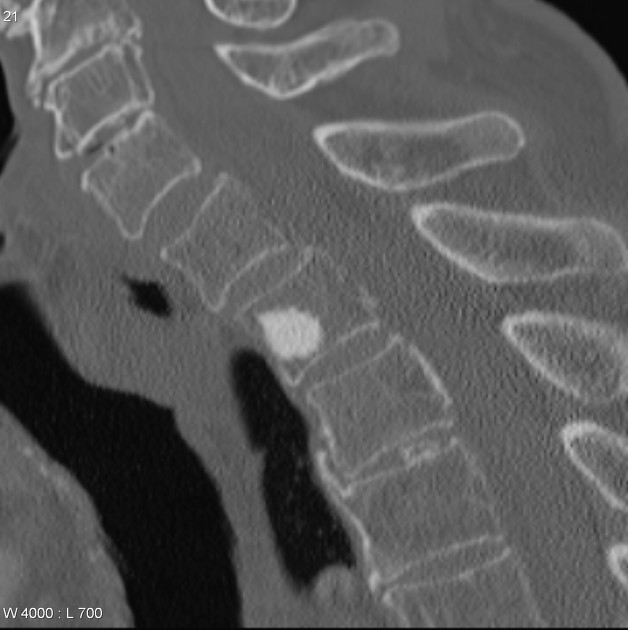
Bone islands are commonly seen as small round or oval foci of homogeneously dense bone within the medullary space. They do not cause cortical destruction or periosteal reaction.
Plain radiograph / CT
The appearance of radiating spicules - "thorny radiation" or "fingers" - at the margins that blend with the surrounding trabeculae is classic, giving a "brush-like" or "stellate" periphery. This is usually best appreciated on CT.
One study has suggested that bone island can be differentiated from bone metastases with a mean attenuation threshold of >885 HU and maximum attenuation of >1060 HU with high sensitivity and specificity 2, but exclusive use of attenuation values in the assessment of sclerotic bone lesions has been discouraged 9.
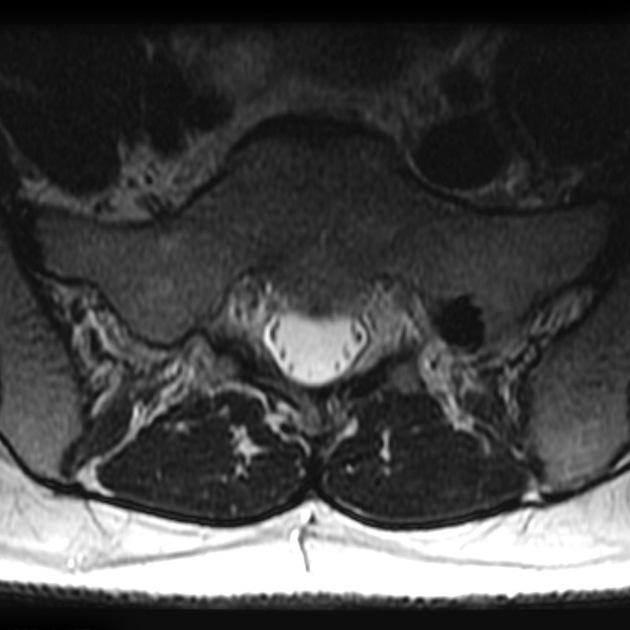
MRI
Bone islands are low signal intensity on all sequences (compatible with compact bone) 10, with no surrounding edema. They do not enhance following contrast administration ref.
Nuclear medicine
There is usually no technetium-99m MDP uptake, and a normal bone scan can exclude sclerotic bone metastases or osteosarcoma. However, low-grade scintigraphic activity has sometimes been reported in histologically proven bone islands, particularly if the lesion is >1 cm 3.
Treatment and prognosis
Sometimes a slow increase in size is seen in bone islands over time 10. Consider biopsy if the lesion grows 50% in one year or 25% in 6 months 4.
Differential diagnosis
In the vast majority of cases, bone islands have a pathognomonic appearance. Larger lesions may sometimes pose a diagnostic dilemma, particularly in the setting of known malignancy.
Imaging differential considerations include:
-
HU measurements may be used as an adjunct (see plain radiograph / CT section above)
may exhibit aggressive features
low-grade osteosarcoma










 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.