
Conventional chondrosarcomas are locally aggressive and malignant cartilagineous or chondrogenic neoplasms and are the most common form of chondrosarcoma 1. Conventional chondrosarcomas can be primary or secondary and are traditionally categorized according to their location within the bone into central and peripheral chondrosarcomas 2. Both central and peripheral chondrosarcomas are histologically similar and are characterized by three histological grades (see chondrosarcoma grading).
To reflect more on the different prognoses and the metastatic potential of those entities the WHO has classified them into the following four entities 3,4:
central atypical cartilaginous tumors/chondrosarcoma grade 1 (ACT/CS1)
secondary peripheral atypical cartilaginous tumors/chondrosarcomas grade 1 (ACT/CS1)
On this page:
Terminology
The term conventional intramedullary chondrosarcoma has been used for central chondrosarcomas, low-grade, intermediate and high-grade.
Epidemiology
Conventional chondrosarcomas make up more than 85-90% of all chondrosarcomas 1,5-7. The relative incidence of conventional chondrosarcomas has been estimated at almost 9 per million about a decade ago with increasing incidence compared to the 1990s. This increase has been attributed to aging and increased use of diagnostic imaging 5.
Conventional chondrosarcomas in general are mainly found in the adult population and most are found in the 3rd to 6th decade. However patients with secondary chondrosarcomas, that is, those arising in the periphery from a pre-existing osteochondroma or centrally from a pre-existing enchondroma e.g. in enchondromatosis are usually up to 1-2 decades younger 4.
The majority (>85%) of conventional chondrosarcomas are primary central chondrosarcomas, whereas a minority (<15%) arise from the cartilage cap of a pre-existing osteochondroma 1,4. Low-grade chondrosarcomas are much more common than intermediate and high-grade tumors 5.
Associations
Secondary conventional chondrosarcomas are associated with the following conditions:
Diagnosis
A provisional diagnosis can be often made by a combination of clinical information, the location of the tumor and imaging features including the size of the cartilaginous cap 4. Tumor grading might require histology 1,4.
Clinical presentation
Typical clinical symptoms are swelling and pain, that might be long-standing and worse at night 1. They might present as a large mass and some tumors might present with a pathological fracture.
Pathology
Conventional chondrosarcomas are aggressive cartilage matrix-forming tumors 1. Based on their etiology they can be subdivided into primary and secondary chondrosarcomas depending on whether they develop in the absence of a precursor lesion or from a pre-existing benign lesion such as an enchondroma or osteochondroma 4,8. Peripheral osteochondromas are secondary chondrosarcomas 1-4.
Etiology
Individuals with enchondromatosis or osteochondromas are at risk to develop secondary chondrosarcomas 1.
Location
The localization of central and peripheral chondrosarcomas is not only different within the bone, but also varies slightly throughout the skeleton:
Central chondrosarcomas arise from an intramedullary location and are more commonly found in the long tubular bones and the pelvis and less commonly the ribs 4.
Peripheral chondrosarcomas arise at the bony surface from the cartilaginous cap of pre-existing osteochondromas and are most frequently found in the pelvis, scapula and ribs within the axial skeleton and the femur and tibia within the appendicular skeleton 4.
Macroscopic appearance
Macroscopically, conventional chondrosarcomas are cartilaginous tumors with a lobular translucent bluish-white appearance. Depending on whether they are central or peripheral their location within bone is different.
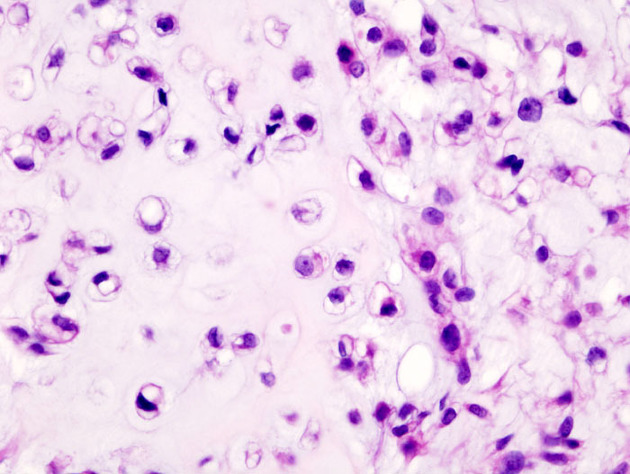
Microscopic appearance
Histologically central and peripheral conventional chondrosarcomas are similar and characterized by the following features 1,8:
cartilaginous matrix-producing tumor
coarse and irregular calcifications
lobular pattern
The presence of mitoses and nuclear pleomorphism indicates intermediate or high-grade chondrosarcoma 4.
Immunophenotype
Immunohistochemistry stains are usually reactive for S100 4.
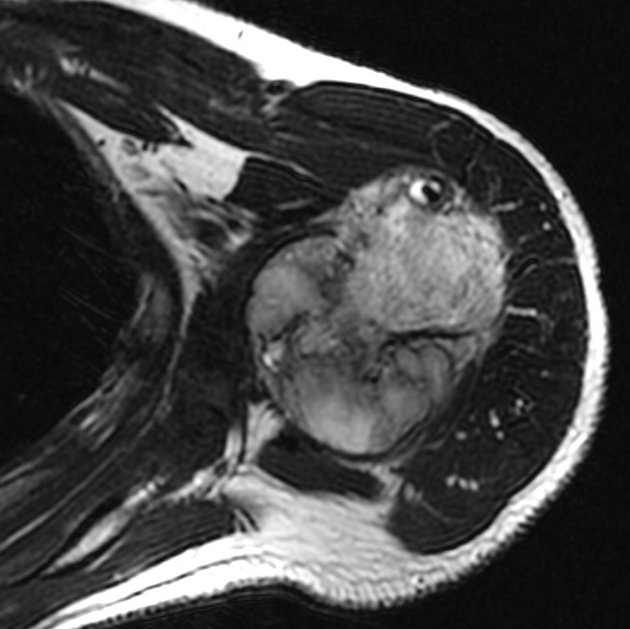
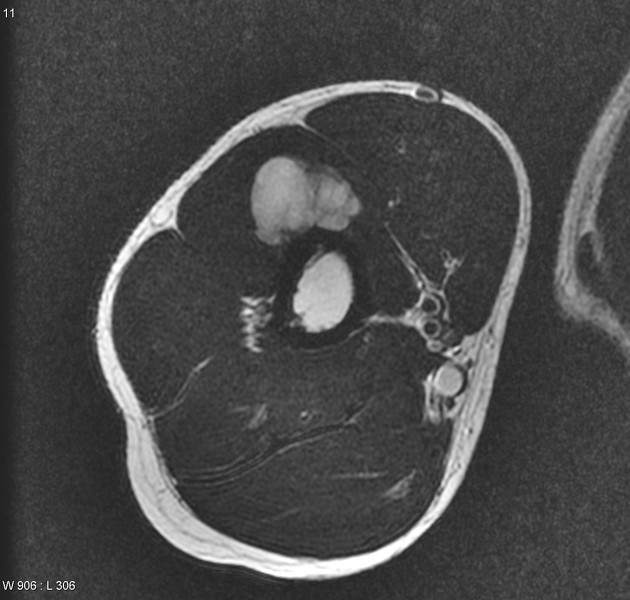
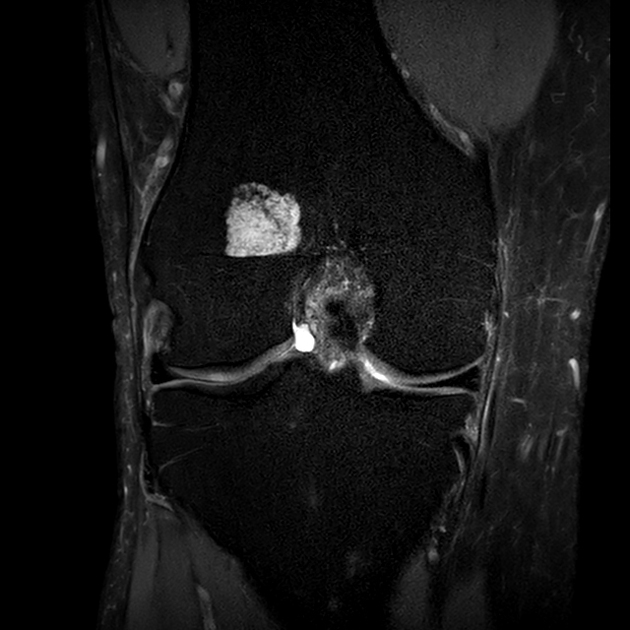
Radiographic features
For imaging findings please refer to the respective articles (see above) or for a general overview of the article chondrosarcoma.
History and etymology
Chondrosarcomas were first described and already categorized into central and peripheral tumors by the American bone pathologists Louis Liechtenstein and Henry Lewis Jaffe in 1939 2.
Conventional chondrosarcomas have been separated since the fourth edition of the WHO classification of bone tumors in 2013 into low-grade chondrosarcomas and intermediate and high-grade chondrosarcomas grade 2 and 3 reflecting the different prognoses and the metastatic potential of the two entities 3,8.
Differential diagnosis
-
low-grade conventional chondrosarcomas can be challenging to distinguish from an enchondroma, as both grow in a nodular pattern and result in scalloping of the inner surface of the cortex
scalloping of greater than two-thirds of the cortical thickness, cortical breach and soft tissue mass beyond the confines of the bone are useful distinguishing features
see article: enchondroma vs. chondrosarcoma




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.