
Hepatic solitary fibrous tumors are rare mesenchymal tumors.
On this page:
Terminology
Historically, hepatic solitary fibrous tumors were known as hepatic hemangiopericytomas, however this term has now been abandoned.
Epidemiology
Fewer than 60 cases of hepatic solitary fibrous tumor have been reported in the literature. Female predominance (~70%). There is a mean age of 52 years at presentation, but a wide range of incidence (16-84 years).
Clinical presentation
If the patient is symptomatic at all, the presentation is usually mild and non-specific, including abdominal pain, bloating, and dyspepsia.
Hypoglycemia has been reported in some patients, presumably a paraneoplastic syndrome.
Pathology
Microscopic appearance
These tumors demonstrate high cellular proliferation of spindle cells arranged in a storiform pattern.
Immunophenotype
CD34: positive
vimentin: positive
Bcl-2: positive
SM-actin: negative
Radiographic features
A prospective diagnosis of hepatic solitary fibrous tumor is not usually possible because imaging features are usually relatively non-specific. Intratumoral necrosis has been reported in a few lesions. Benign tumors cannot be reliably be differentiated from malignant tumors.
CT
-
nonspecific enhancing mass
heterogeneous enhancement has been reported
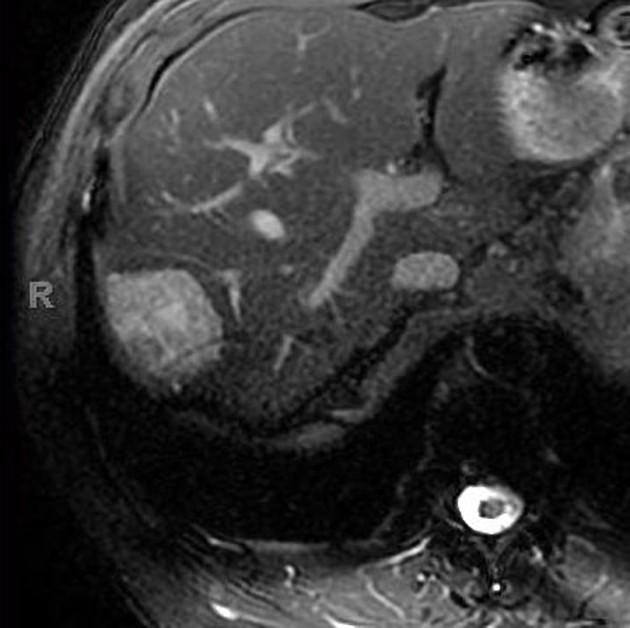
MRI
T1: hypointense
T2: heterogeneous appearance
T1 C+ (Gd): heterogeneous enhancement, depending on the relative amounts of cellular and collagen components
Nuclear Medicine
FDG-PET: avid FDG uptake 5
Treatment and prognosis
Most recorded hepatic solitary fibrous tumors are benign, but it is possible for them to exhibit malignant behavior 2. Some think that malignant foci may exist in biopsy-benign tumors, and the risk of malignancy is estimated at ~10% 1.
Given the rarity of the tumor, no standard treatment exists. Partial hepatectomy has been performed for some lesions, given the concern for occult malignancy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.