
Right-sided aortic arch is a type of aortic arch variant characterized by the aortic arch coursing to the right of the trachea. Different configurations can be found based on the supra-aortic branching patterns, with the two most common patterns being the right-sided aortic arch with mirror image branching and the right-sided aortic arch with aberrant left subclavian artery (ALSA).
On this page:
Epidemiology
A right-sided aortic arch is thought to occur in approximately ~0.1% (range 0.05-0.2%) of the population. There is a significant association with 22q11.2 deletion syndrome (DiGeorge syndrome) 14.
Clinical presentation
The majority of the patients are asymptomatic and it is discovered incidentally. However, it causes symptoms when associated with other vascular anomalies (vascular ring) due to compression of the esophagus and/or trachea.
Pathology
Types
Right-sided arches can be divided into at least three types. Please note that the numbering of the types varies from publication to publication; therefore, the abnormality should be described rather than merely numbered 1,7,11-13.
-
type I: right-sided aortic arch with mirror image branching
sometimes reported as the most common, accounting for up to 59% of all right-sided arches 11. In most of the literature, though, it is reported as less common than type II 1
occurs from interruption of the dorsal segment of the left arch between the left subclavian artery and the descending aorta, with regression of the right ductus arteriosus in the hypothetical double aortic arch
in this variant, the left brachiocephalic trunk arises first, followed by the right common carotid and right subclavian arteries
-
usually associated with cyanotic congenital heart disease, including
-
type II: right-sided aortic arch with aberrant left subclavian artery
common 1, at least accounting for 39.5% of all right-sided arches 11
associated with a Kommerell diverticulum 11
occurs from interruption of the dorsal segment of the left arch between the left common carotid and left subclavian arteries with regression of the right ductus arteriosus in the hypothetical double aortic arch
in this variant, the left common carotid artery arises first, followed by the right common carotid, right subclavian, and then left subclavian arteries
rarely symptomatic and is therefore usually incidental, although it can rarely cause esophageal and/or tracheal compression 10
rarely associated with other cardiovascular abnormalities
-
type III: right-sided aortic arch with isolation of the left subclavian artery 1,6
rarest type: 0.8% 11
results from interruption of the left arch at two levels, with one level between the left common carotid and left subclavian arteries and the other level distal to the attachment of the left ductus
may be associated with congenital subclavian steal syndrome and vertebrobasilar insufficiency
can be rarely associated with congenital heart disease
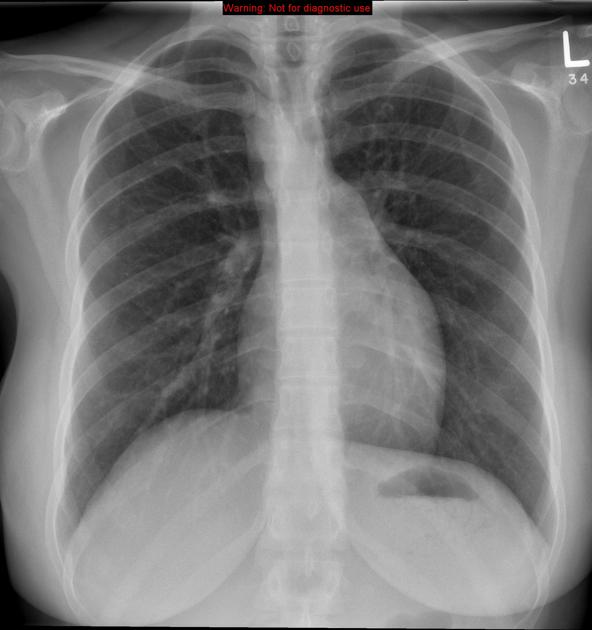
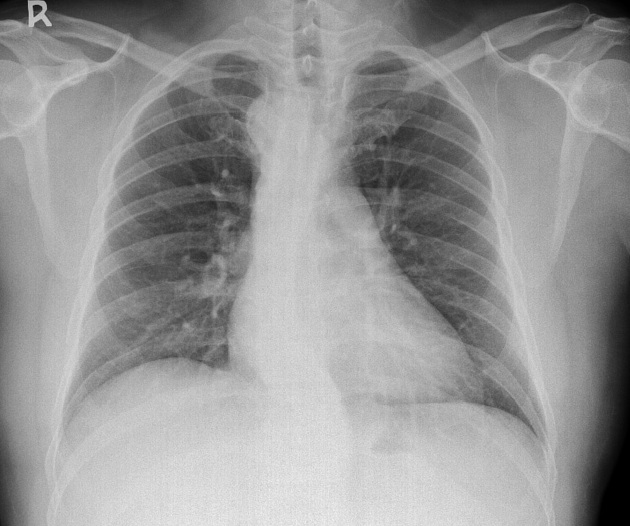
Radiographic features
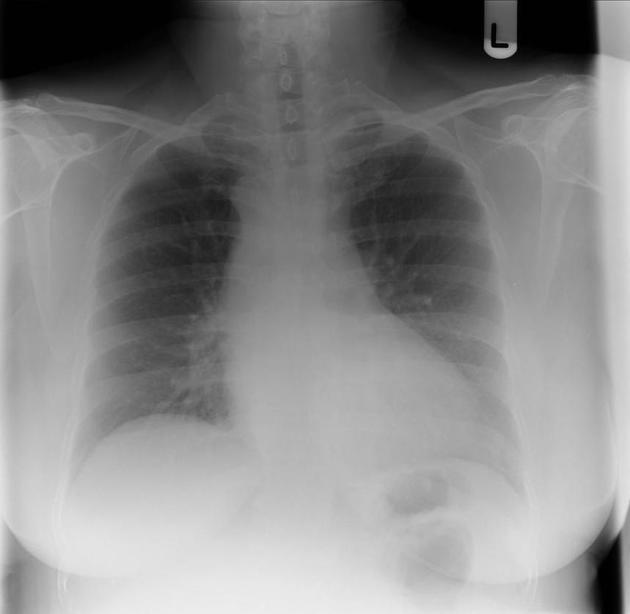
Plain radiograph
left aortic contour is absent
tracheal bowing to the left at the level of the right aortic arch
soft tissue indentation on the right side of the distal trachea
right-sided descending aorta
The right arch is often seen as high riding and projecting as a mass in the right paratracheal region 4.
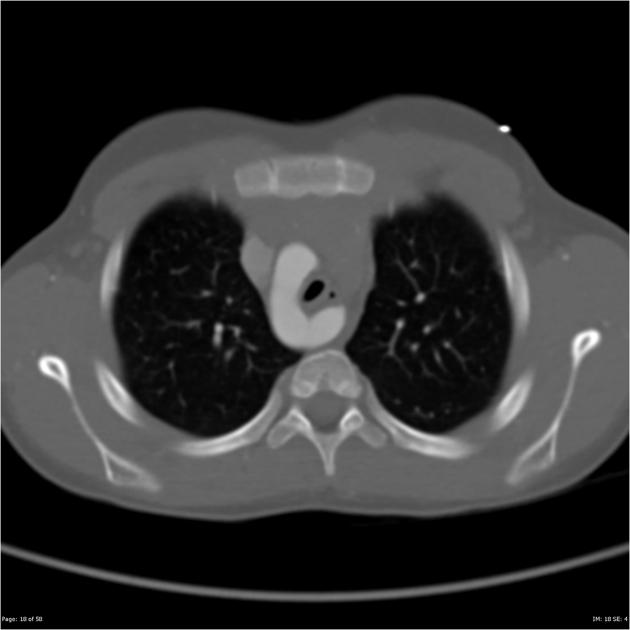
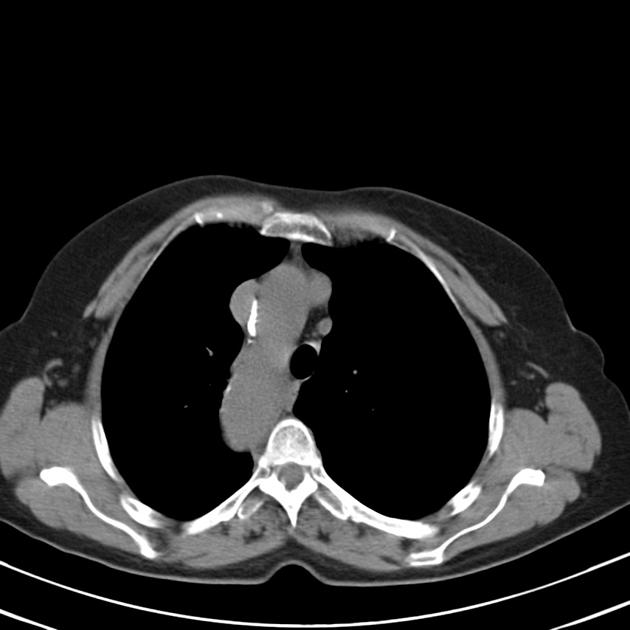
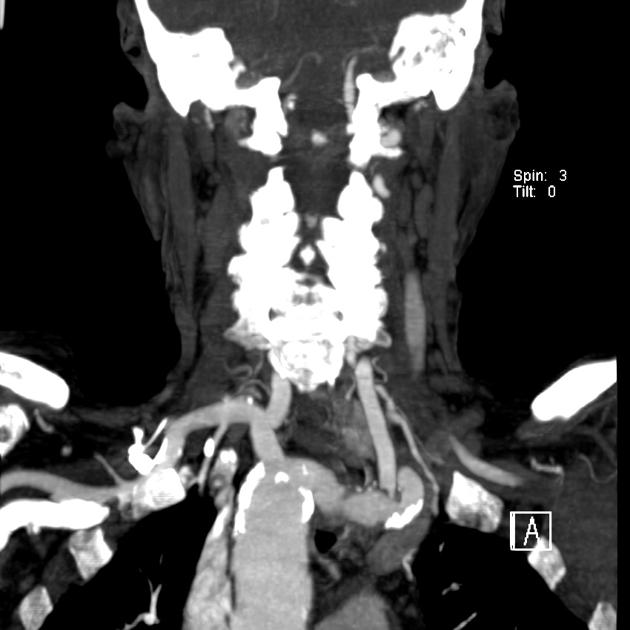
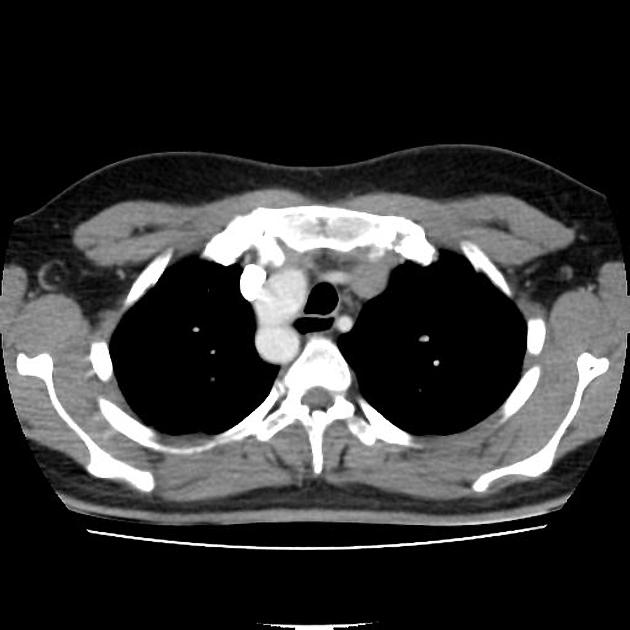
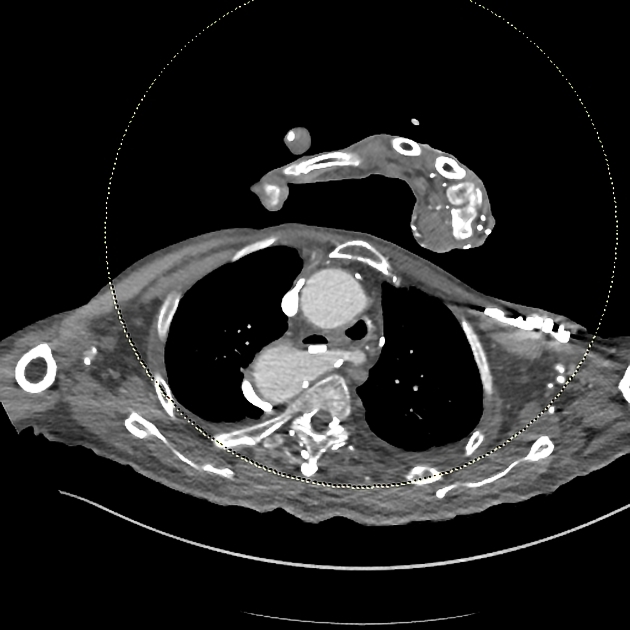
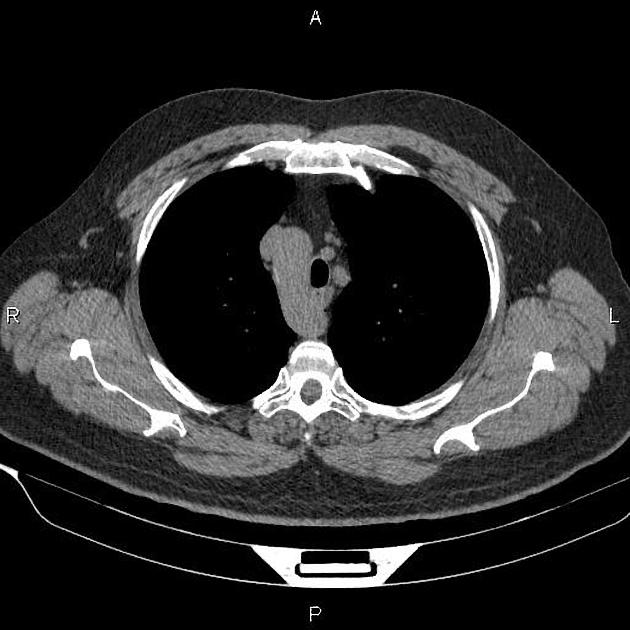
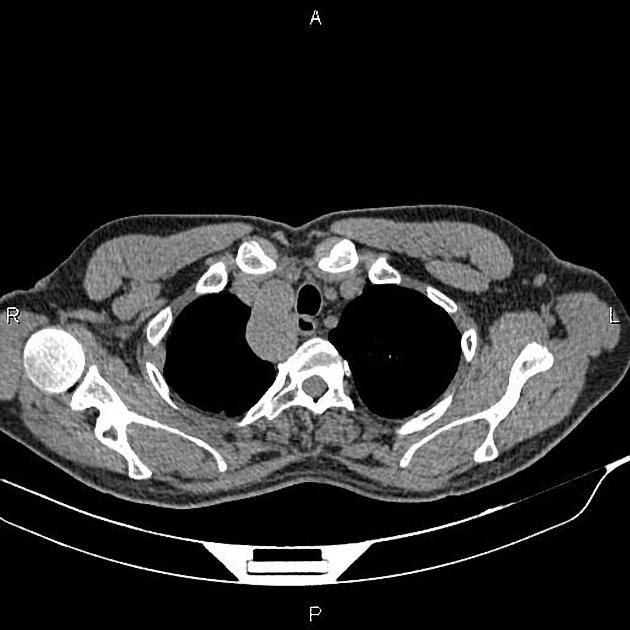
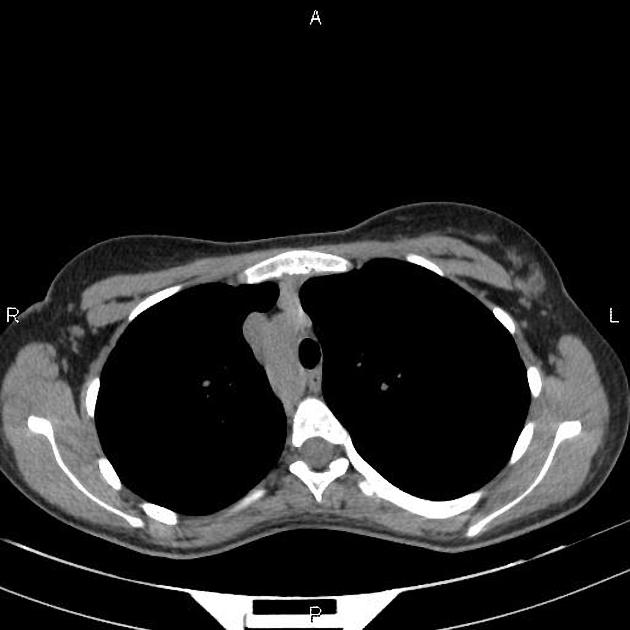
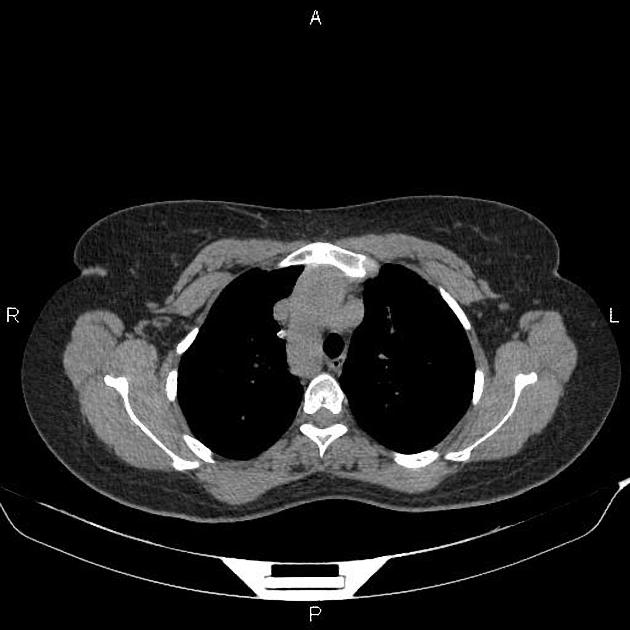
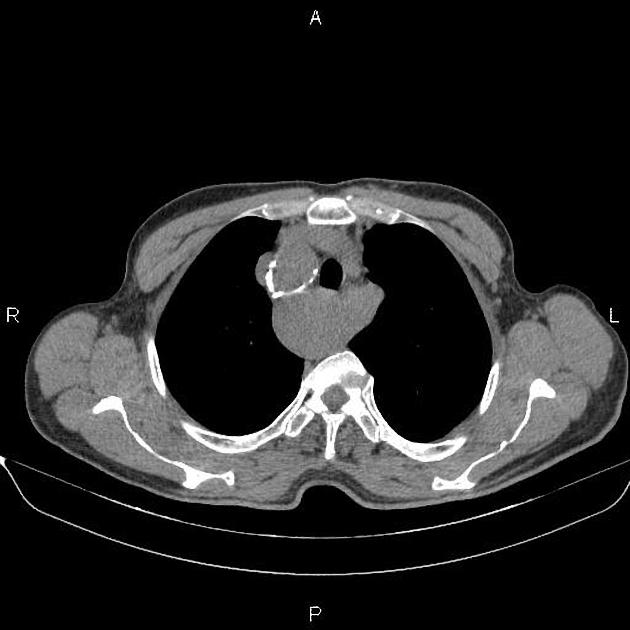
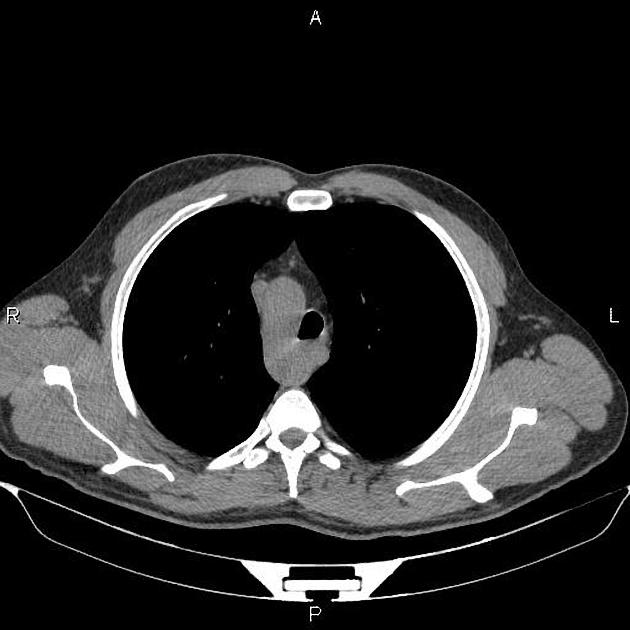
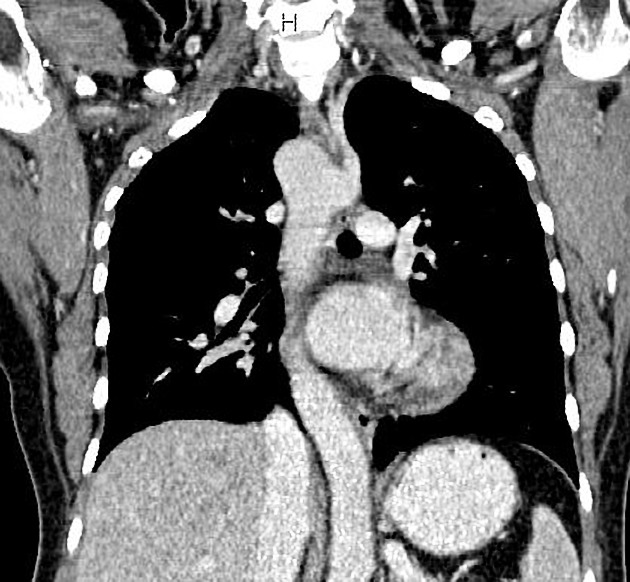
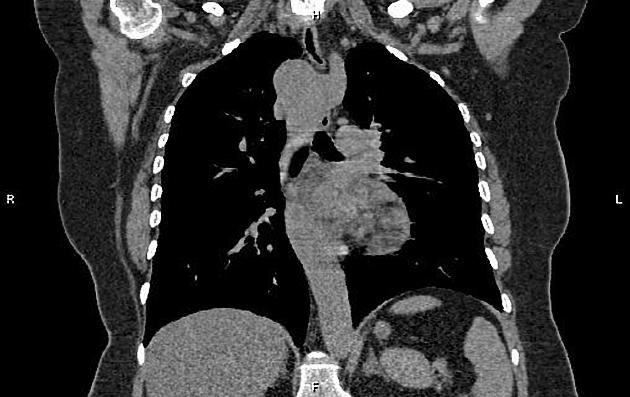
CT/MRI
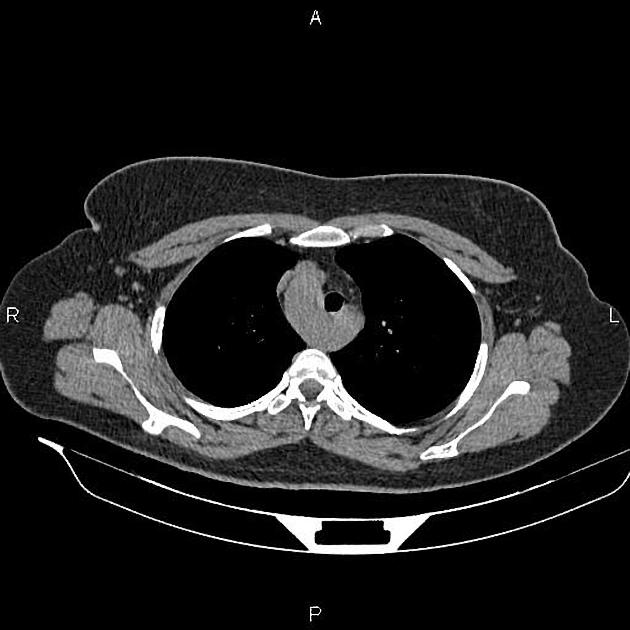
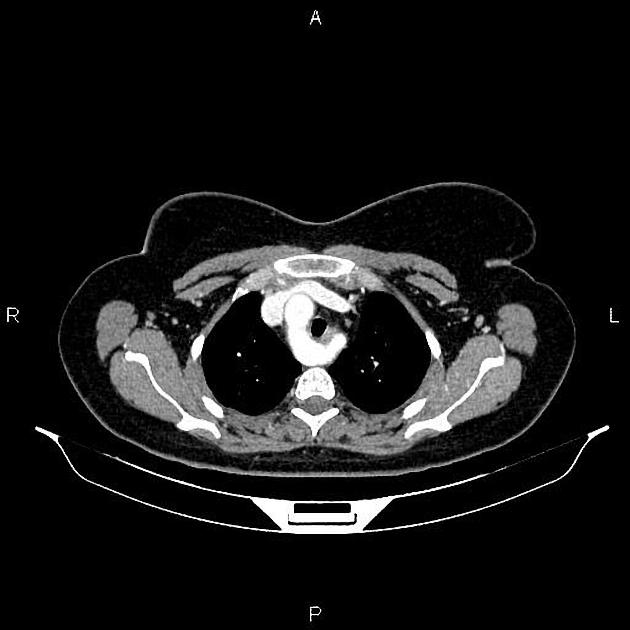
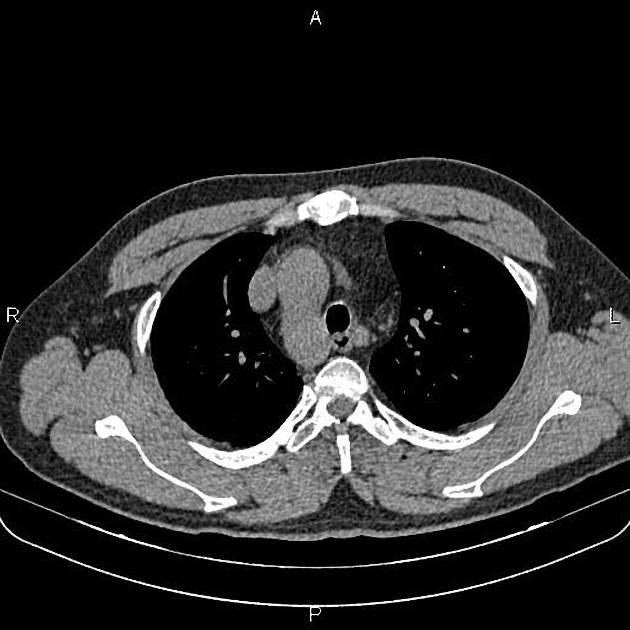
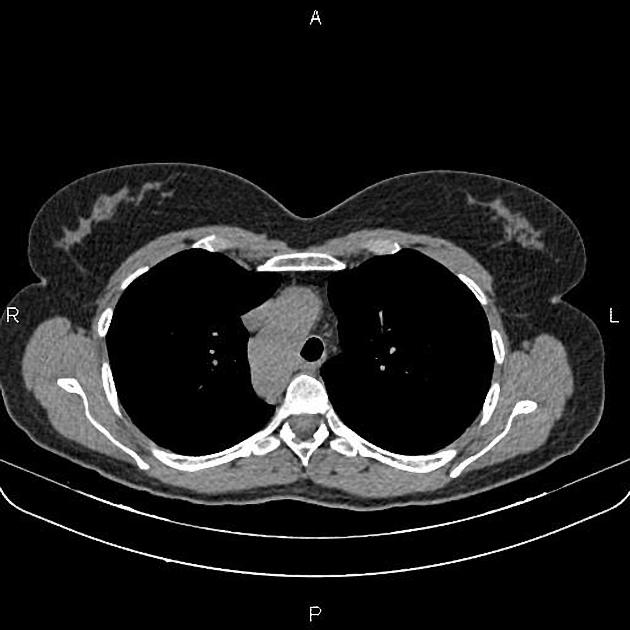
Cross-sectional imaging with CT or MRI allows direct visualization of arch anatomy and with dedicated angiographic techniques (MRA or CTA) excellent demonstration of the lumen can be achieved.


















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.