
A portal venous varix (plural: portal venous varices) refers to a segments of aneurysmal or variceal dilatation of the portal vein.
On this page:
Epidemiology
Portal venous varices are extremely rare, representing only 3% of all aneurysms of the venous system. They are still, however, the most common visceral varix 8.
Clinical presentation
Most patients are asymptomatic but may present with nonspecific abdominal pain as a major symptom 2-4. A large varix may cause pain, jaundice, or rarely, gastrointestinal bleeding.
Pathology
Both congenital and acquired causes have been proposed. Acquired causes may include 2,3:
- portal hypertension: could be contributory but is not essential to the development of portal venous system aneurysms; indeed, the majority of patients do not have portal hypertension or chronic liver disease
- necrotizing pancreatitis
- abdominal trauma or surgery
- liver cirrhosis
Location
Majority (~63-77%) tend to be extrahepatic 8.
The most common locations for aneurysms of the portal venous system are 2,3:
- splenomesenteric venous confluence
- main portal vein
- intrahepatic portal vein branches at bifurcation sites
The rarest locations are the splenic, mesenteric, and umbilical veins.
Morphology
They can be either fusiform (~ majority 97% 8) or saccular. The majority tend to be solitary.
Radiographic features
Diagnosis can be made when the portal vein exceeds 20 mm in diameter.
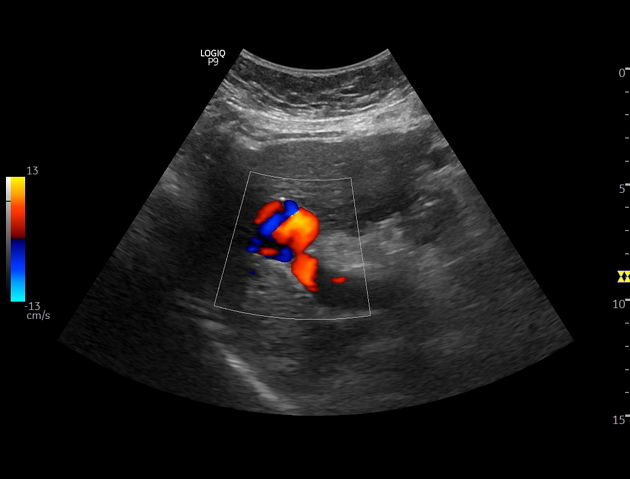
Ultrasound
Color Doppler ultrasound is the most helpful diagnostic tool. Further workup may not be necessary 4. An aneurysm appears on ultrasound as an anechoic mass showing direct luminal continuity with the portal venous system and displays spectral findings characteristic of the portal venous system on color Doppler interrogation 5,6.
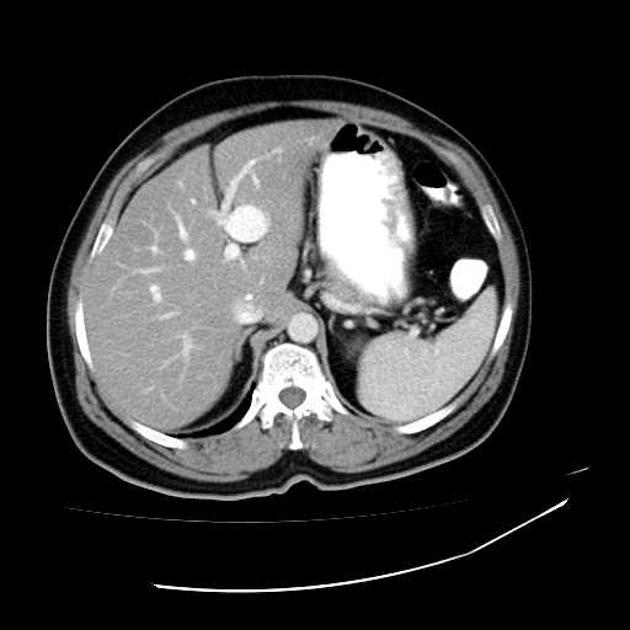
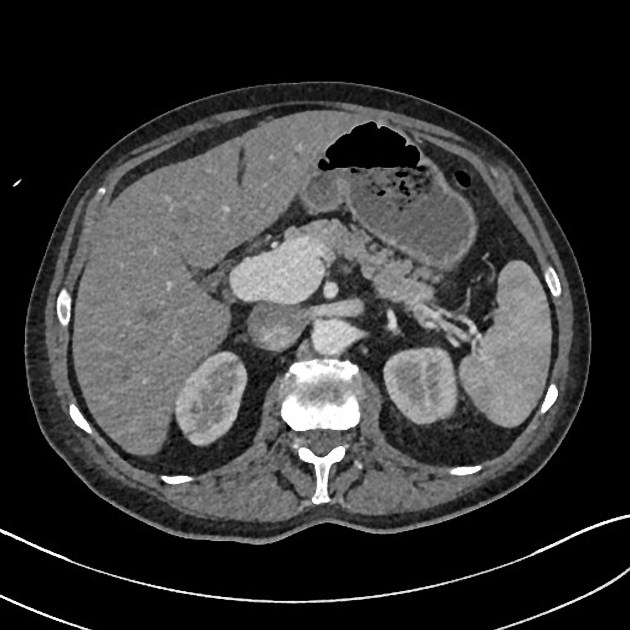
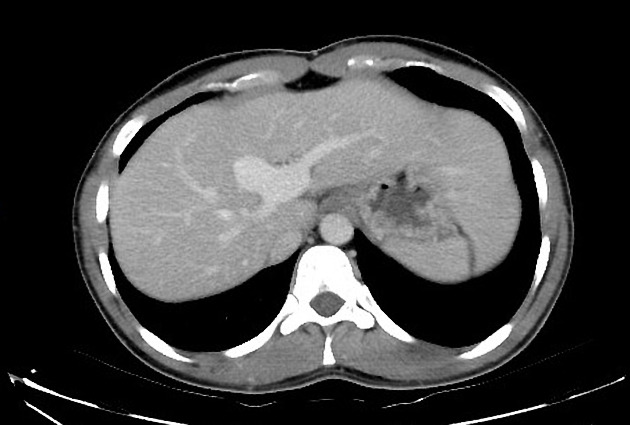
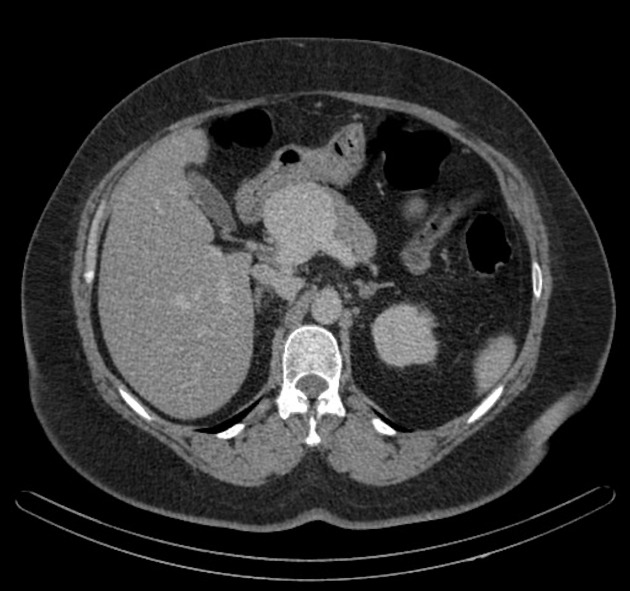
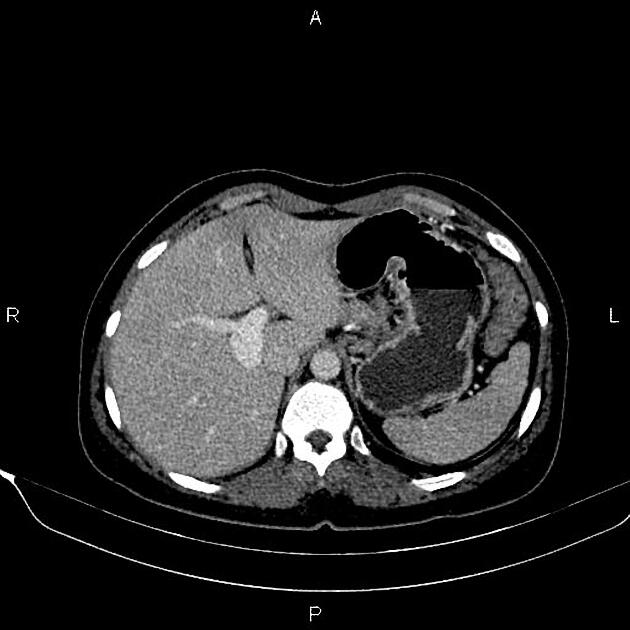
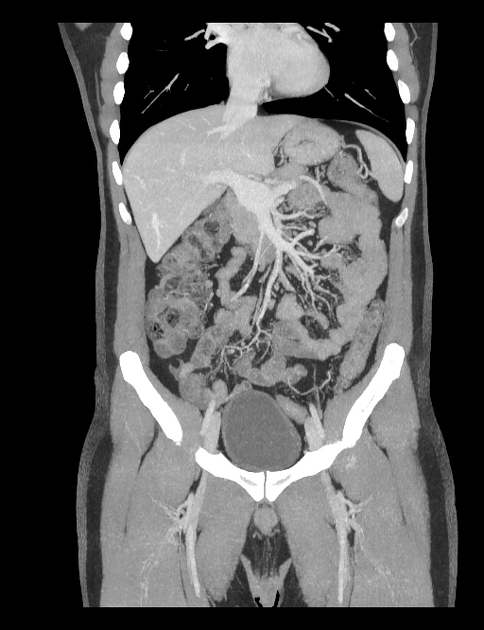
CT
Dynamic helical CT demonstrates simultaneous enhancement with the portal system where a variceal segment may be directly visualized 5,6.
MRI
There is variable signal intensity on T1- and T2-weighted images. In some instances on T1-weighted images, aneurysms can be hypointense owing to the flow-void phenomenon 5.
Treatment and prognosis
Complications
Complications include 2-4:
- thrombosis and distal embolism
- portal hypertension
- rupture
- compression of the duodenum
- compression of the common bile duct causing jaundice, cholestasis, and cholelithiasis
History and etymology
Portal venous varices are thought to have been first described by Barzilai and Kleckner in 1956 9.






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.