
Transsphenoidal basilar skull fractures are a particularly serious type of basilar skull fracture usually occurring in the setting of severe traumatic brain injury and with potential for serious complications including damaging the internal carotid arteries and optic nerves as well as high incidence of dural tear with CSF leak. Venous thrombosis complicates up to 31% of these fractures; as many as 75% of caroticocavernous fistulae will have antecedent skull base fractures.
Pathology
Due to the particulars of the anatomy of the base of skull, fractures that involve the sphenoid sinus tend to extend along a number of predefined pathways 3,4:
Anterior transverse
impact: lateral in the region of the temple
-
coronal fracture plane
extending from the squamous temporal bone
through the base of the anterior clinoid processes anterior to the pituitary fossa
continuing laterally along the contralateral sphenotemporal buttress +/- into the squamous temporal bone
may extend inferiorly to involve the pterygoid processes
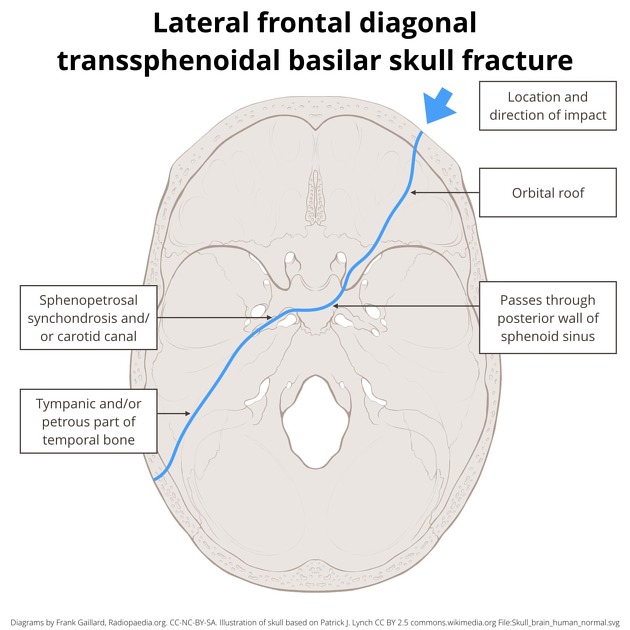
Lateral frontal diagonal
impact: lateral frontal/anterior malar eminence
-
oblique fracture plane
extending from lateral frontal/lateral orbital roof
through the sphenoid sinus
through or adjacent to the contralateral carotid canal into sphenopetrosal synchondrosis
extends as a petrous temporal bone fracture
often associated with maxillary sinus fractures and lateral orbital wall
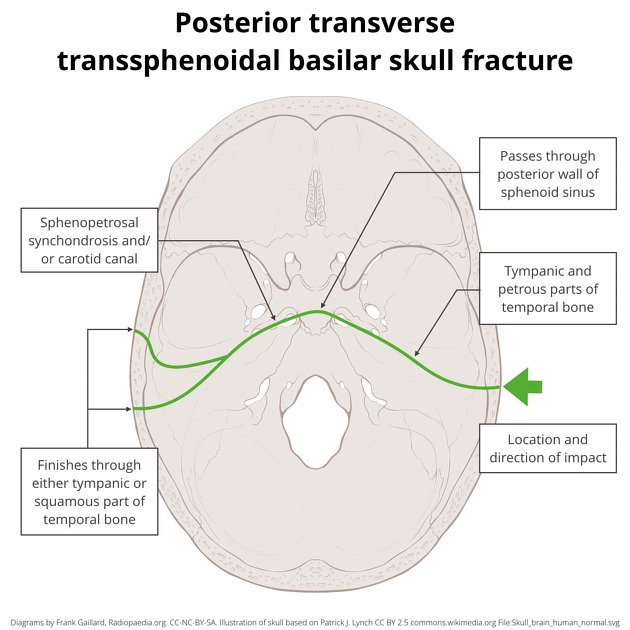
Posterior transverse
impact: lateral, just anterior to the external acoustic meatus
U-shaped fracture comprised of bilateral longitudinal temporal bone fractures (or mixed) united in the midline by a fracture through the posterior wall of sphenoid/clivus
involves sphenopetrosal synchondrosis, foramen lacerum and carotid canal
Mastoid diagonal
impact: posterolateral in the mastoid region
-
oblique fracture
originating in the occipital bone
extending to the jugular foramen and petro-occipital fissure
diagonally passing through sphenoid
into contralateral ethmoid air cells or orbital roof





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.