
Occipital condylar fractures are uncommon injuries usually resulting from high-energy blunt trauma. They are considered a specific type of basilar skull fracture, and importantly can be seen along with craniocervical dissociation.
Treatment of isolated injury is generally conservative, unless there is craniocervical junction instability.
On this page:
Epidemiology
-
relatively uncommon
reported in 3-4% of patients with moderate-severe traumatic brain injuries 3
-
mostly occur in the setting of high-energy trauma 5:
motor vehicle collision (most common)
fall from a significant height
-
reported, but uncommon 5:
pedestrian trauma
assault
rarely with low-energy trauma, e.g. fall from standing in debilitated patient 5
-
may occur as an isolated injury or with additional skeletal injuries 5
+/- associated cervical spine fracture
may be bilateral 5
Clinical presentation
History and examination are unreliable. A high suspicion should be maintained in patients presenting after blunt trauma with any of the following 3,6:
loss of consciousness (low Glasgow coma score)
occipital or neck pain (responsive patients)
impaired craniocervical range of motion
-
neurological deficit:
lower cranial nerve palsy
limb weakness
vertigo
diplopia
Mechanism
Occipital condyle fractures may result from blunt high-energy trauma to the head/neck, especially 3:
axial compression
lateral bending
axial rotation
direct blow
Each occipital condyle articulates along a shallow groove atop each lateral mass of C1 (atlas). This articulation is directly stabilized by 7,8:
atlanto-occipital joint capsule
alar ligaments (dens to each occipital condyle)
Injury to these ligaments may result in instability, particularly in the setting of additional injuries to the major craniocervical ligaments (occipitodental, atlantodental) 7. These ligamentous injuries may also be associated with osseous avulsion fractures at their condylar attachments.
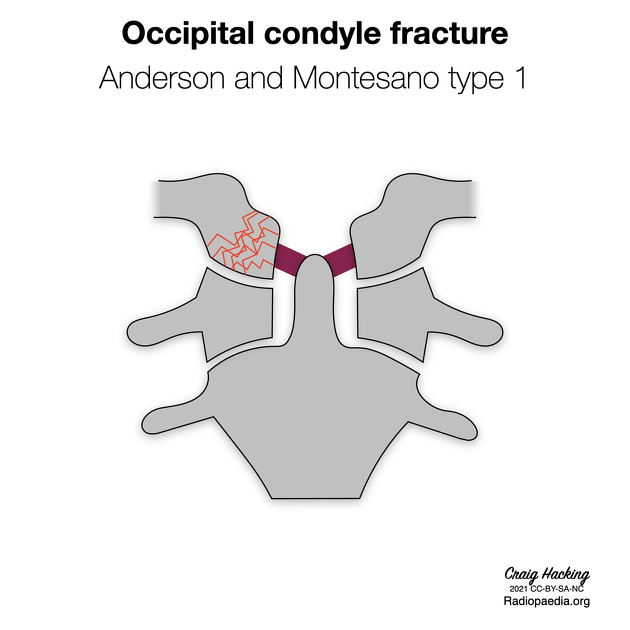
Classification
The classification system widely used for describing occipital condyle fractures is the Anderson and Montesano system 1,2,9. However, as it is purely descriptive, a more clinically-oriented classification has been proposed which incorporates MRI findings and suggested management (see Tuli classification of occipital condyle fractures) 2,5,10.
Radiographic features
The role of imaging is foremost to evaluate for craniocervical dissociation or other catastrophic (e.g. spinal cord) injury, and then to identify and stratify all lesser craniocervical injuries.
Plain radiograph
A lateral cervical spine radiograph is commonly obtained to screen for cervical spine injury in the setting of trauma. Occipital condyle fractures are rarely evident by x-ray 5,6.
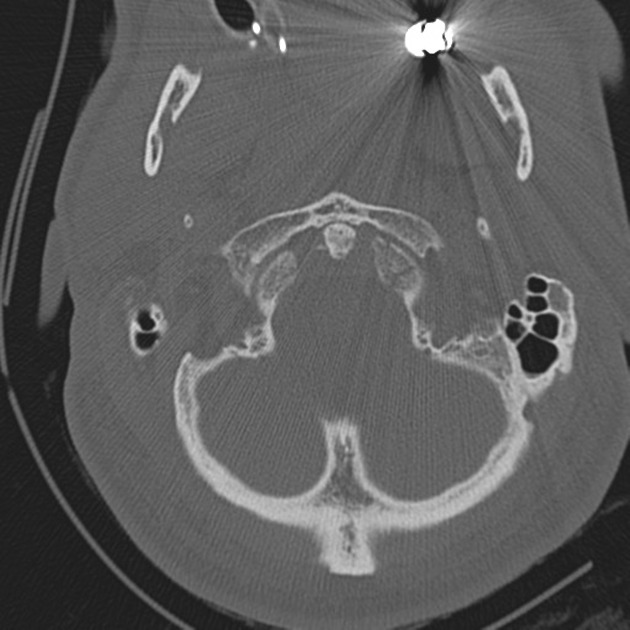
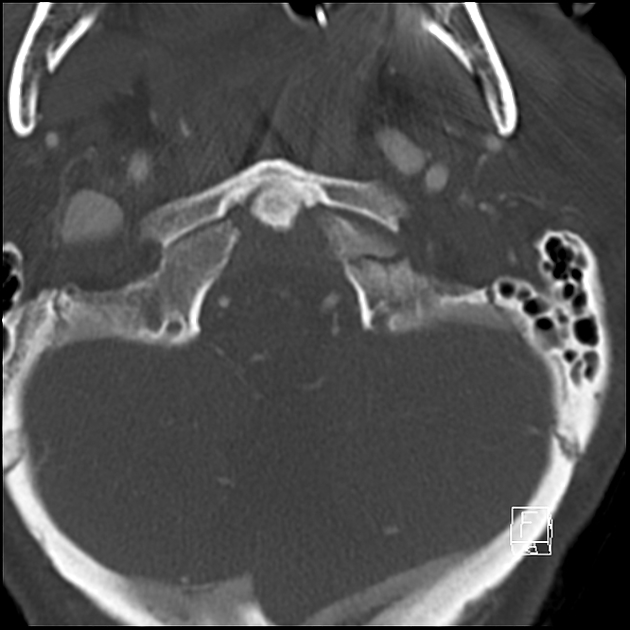
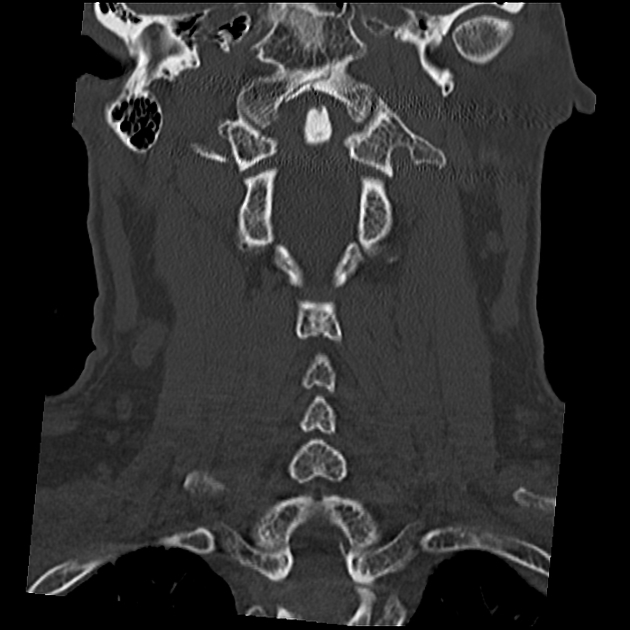
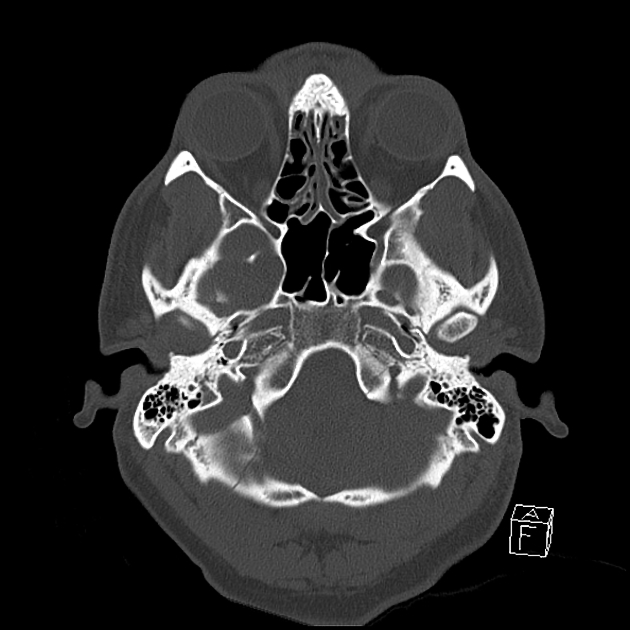
CT
CT is the best modality for identifying an occipital condyle fracture 6. Fractures are best visualized on coronal and sagittal reformatted images.
Important aspects of evaluation include:
-
occipital condyle integrity
comminuted fracture: suggests impaction
curvilinear fracture fragment along medial condyle: suggests avulsion, possible ligamentous injury
-
atlanto-occipital articulation and atlanto-axial joint
alignment: asymmetry in any plane suggests instability (ligamentous injury)
-
joint spaces
occipitoatlantal joint: should be <2 mm 9
atlantoaxial joint: should be <3 mm 5
evaluation for spinal canal narrowing
evaluation for cervicomedullary or spinal hemorrhage
-
other fractures
skull base
C1, C2
MRI
MRI is commonly performed after a craniocervical injury is initially identified. The primary purpose is to exclude spinal cord injury, although other specific indications include:
evaluate for suspected major ligamentous injury
surgical treatment planning in the setting of known instability
high-suspicion patients who cannot be reliably examined within 48 hours: even with initial normal CT
MR findings include:
-
direct findings of condyle fracture
cortical disruption, fragment displacement
marrow edema
-
occipito-atlantal joint effusion
effusion itself may be normal 5
joint space widening and hemorrhage (fluid-fluid level) are more specific for significant traumatic injury 2
-
alar ligament injury
disruption, edema
there may be additional adjacent ligamentous injuries, e.g. tectorial membrane, anterior and posterior atlanto-occipital membranes, prevertebral or nuchal ligaments 6
retrodental hemorrhage 6
The following limitations of MRI should be considered 5:
CT generally is more sensitive for fractures
CT is better for assessing craniocervical alignments
-
MR cannot exclude craniocervical instability
limited sensitivity for ligament injury
individual ligaments not often discernible
Treatment and prognosis
The most important factor in the management of craniocervical junction injuries is the status of the stabilizing occipitoatlantoaxial ligaments.
In the absence of obvious instability ligament disruption, most occipital condyle fractures are managed non-operatively with external stabilization 7. Isolated unstable fractures may be treated by posterior occipitocervical fusion 7.
When considered according to Anderson and Montesano types, type I and II injuries are generally stable because the alar ligament and tectorial membrane are preserved, while type III is potentially unstable ref.
Non-surgical management typically results in mild residual impairment 8.
Differential diagnosis
ossification of ligament of odontoid process 2
occipital condyle syndrome: atraumatic syndrome with similar clinical features, often due to metastatic malignancy






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.