
Scapula fractures are uncommon injuries, representing ~3% of all shoulder fractures.
On this page:
Epidemiology
Associations
Scapular fractures are often associated with other injuries due to the high energy trauma that is usually the underlying cause:
- clavicle fracture
- rib fracture
- sternal fracture
- spinal fracture
- pneumothorax and/or pulmonary contusion
- brachial plexus injury
Pathology
Mechanisms of injury
- requires high energy trauma (e.g. motor vehicle accidents account for 50% of scapular fractures)
- direct trauma to the shoulder region
- indirect trauma through falling on outstretched hand
- non-accidental injuries in children
Radiographic features
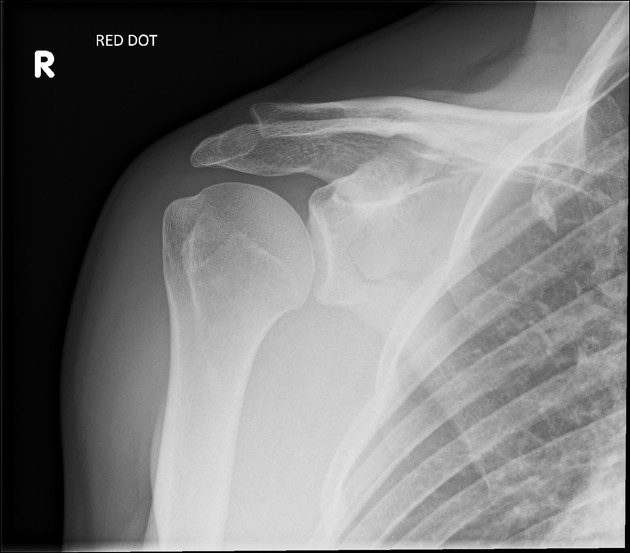
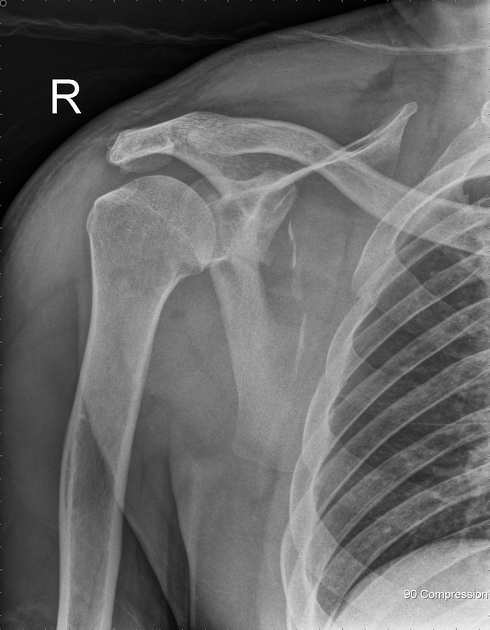
Plain radiograph
Requires trauma series views to demonstrate the fractures due to the superimposition of the shoulder girdle and thoracic cage.
Radiographic series includes:
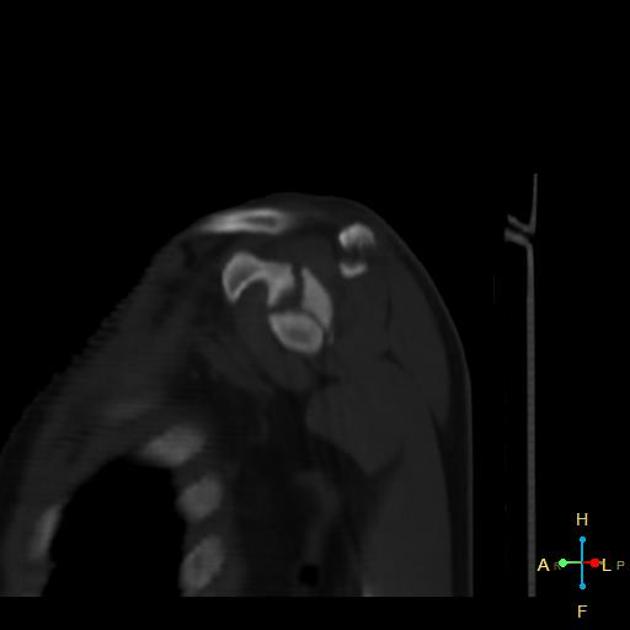
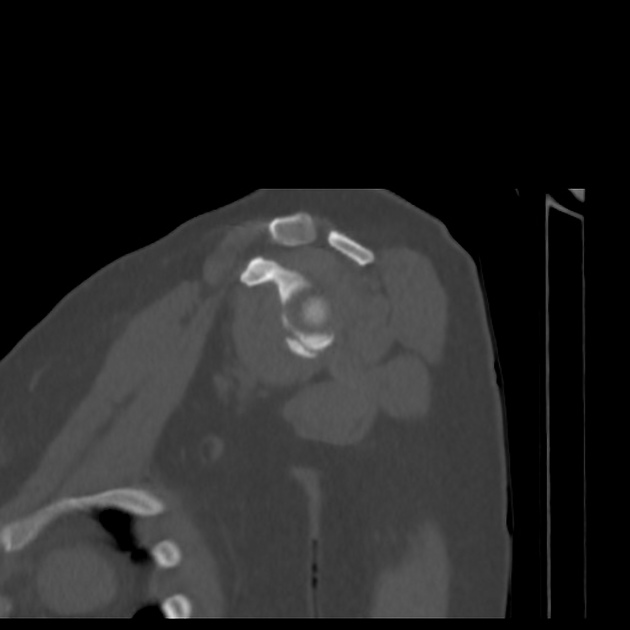
CT
- standard for diagnosis and evaluation of the fracture and its associated injuries
- axial scan with coronal, sagittal and 3D reconstructions are used in the assessment of scapular injuries
Classification
-
intra-articular glenoid fracture
- type I: avulsion of anterior glenoid margin
- type II: transverse or oblique fracture through glenoid fossa exiting inferiorly
- type III: oblique fracture through glenoid fossa exiting superiorly and associated with acromioclavicular joint injury
- type IV: transverse fracture exiting through the medial scapular border
- type V: combination of type II and type IV
- type VI: comminuted glenoid fracture
-
extra-articular glenoid fracture
- type I: glenoid neck fracture without clavicular fracture
- type II: glenoid neck fracture with clavicular fracture and acromioclavicular dislocation
-
coracoid process fracture
- type I: fracture proximal to the coracoclavicular ligament
- type II: fracture distal to the coracoclavicular ligament
-
acromial fracture
- type I: minimally displaced
- type II: displaced but does not reduce subacromial space
- type III: displaced and narrow the subacromial space
Differential diagnosis
- os acromiale and other accessory ossicles of the scapula












 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.