
The axillary lymph nodes, also known commonly as axillary nodes, are a group of lymph nodes in the axilla that receive lymph from vessels that drain the arm, the walls of the thorax, the breast and the upper walls of the abdomen.
Gross anatomy
There are five axillary lymph node groups, namely the lateral (humeral), anterior (pectoral), posterior (subscapular), central and apical nodes. The apical nodes are the final common pathway for all of the axillary lymph nodes.
Lateral (humeral) lymph nodes
location: posteromedial to axillary vein
receives: lymph from most of the upper limb
drains into: central, apical and deep cervical nodes
Anterior (pectoral) lymph nodes
location: inferior border of pectoralis minor, near lateral thoracic vessels
receives: lymph from skin and muscles of the supraumbilical anterolateral body wall, breast
drains into: central and apical nodes
Posterior (subscapular) lymph nodes
location: along subscapular vessels on inferior margin of the posterior axillary wall
receives: lymph from skin and muscles of the posterior and inferior body wall
drains into: central and apical nodes
Central lymph nodes
location: fat of the axilla
receives: the above mentioned lateral, anterior and posterior lymph node groups
drains into: apical nodes
Apical (terminal) lymph nodes
location: posterior and superior to pectoralis minor, towards the axillary vein
receives: lymph from cephalic vein nodes, upper peripheral breast, the above mentioned central nodes
drains into: subclavian trunk (may drain into jugulosubclavian venous trunk, subclavian vein, jugular lymphatic trunk, right lymphatic duct (left into thoracic duct), inferior deep cervical nodes)
Lymphatic pathways
Lymphatics pass around the edge of the pectoralis major and reach the pectoral group of axillary nodes. Routes through or between the pectoral muscles may lead directly to the apical nodes of the axilla. Lymphatics follow the blood vessels through the pectoralis major and enter the parasternal (internal thoracic) nodes.
Connections may lead across the median plane and hence to the contralateral breast. Lymphatics may reach the sheath of the rectus abdominis muscle and the subperitoneal and subhepatic plexuses.
There is free communication between nodes below and above the clavicle and between the axillary and cervical nodes.
Surgical levels
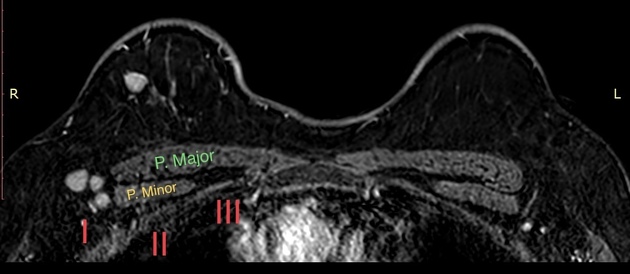
There are three surgical levels of axillary lymph nodes which use the pectoralis minor muscle as the key landmark; this classification was developed by an American pathologist, John W Berg 7:
level I: below the lower edge of the pectoralis minor muscle
level II: underneath/posterior to the pectoralis minor muscle
level III: above/medial to the pectoralis minor muscle
The lymphatic drainage of the breast is of great importance in the spread of carcinoma and about three-quarters of it is to the axillary nodes.
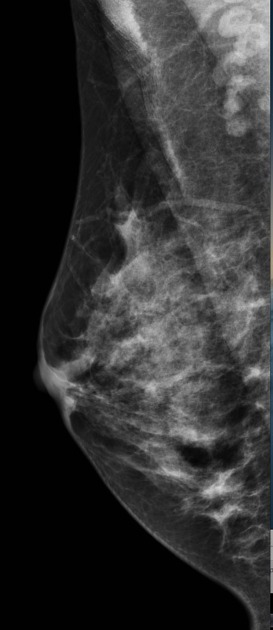
Radiographic appearance
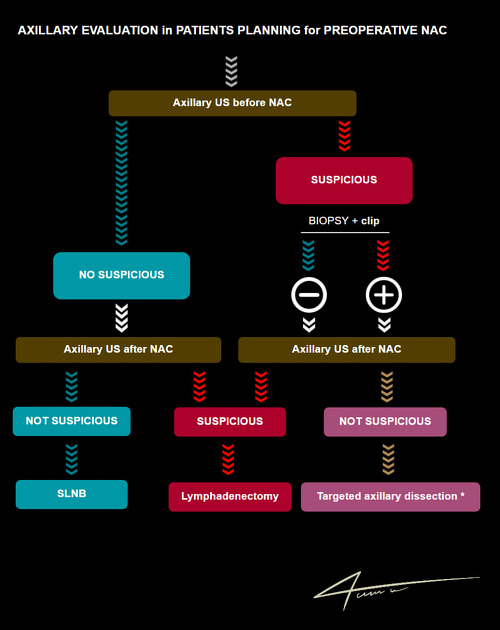
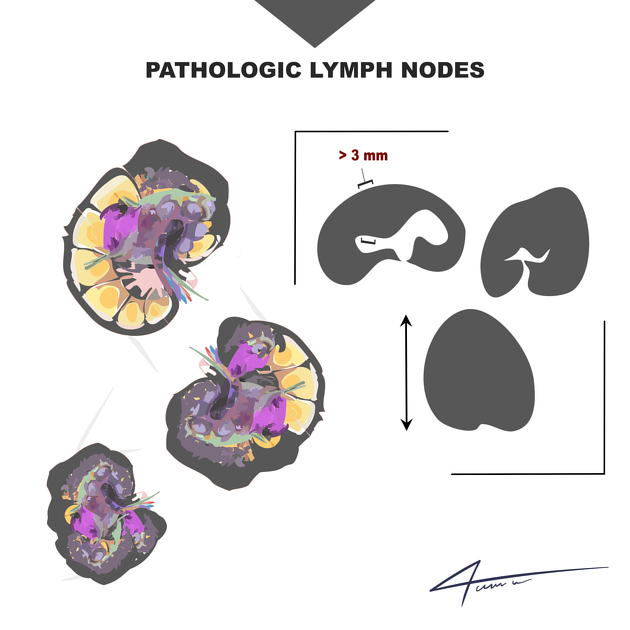
In breast imaging, there are several schools of thought as to when to biopsy axillary nodes. Many suggest biopsying when the following features are present:
loss or disruption of central fatty hilum
loss or pericapsular fat line
parenchymal cortical thickness greater than 2.5 mm
presence of abnormal color flow
irregular outer margins






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.