
Sclerotic or osteoblastic bone metastases are distant tumor deposits of a primary tumor within bone characterized by new bone deposition or new bone formation.
On this page:
Epidemiology
Bone metastases are the most common bone malignancy, with sclerotic bone metastases being less common than lytic bone metastases.
Diagnosis
The diagnosis is usually established by a combination of imaging and the known presence of a primary tumor associated with sclerotic bone metastases. It can also be proven histologically.
Pathology
Osteoblastic bone metastases are characterized by increased bone formation 2. However, the exact mechanism that leads to osteoblastic formation is not entirely elucidated. Several tumor-derived growth factors are assumed to increase osteoblast activity while osteoclast activity is restricted 3,4.
Etiology
Sclerotic bone metastases can arise from several different primary malignancies, including 1-3:
prostate carcinoma (most common)
breast carcinoma (may be mixed)
mucinous adenocarcinoma of the gastrointestinal tract (e.g. colon carcinoma, gastric carcinoma)
Hodgkin lymphoma (e.g. ivory vertebra)
Radiographic features
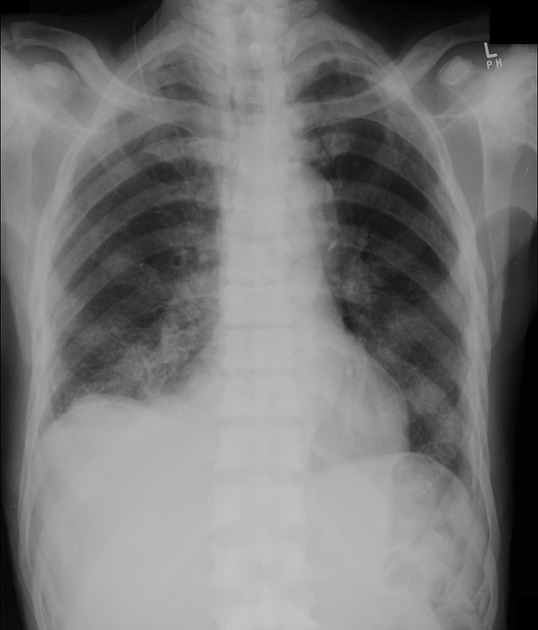
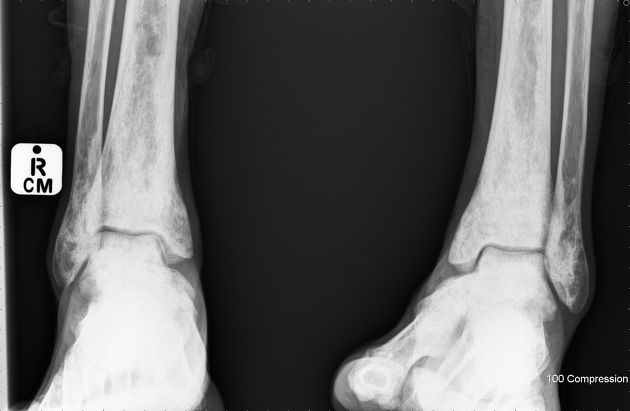
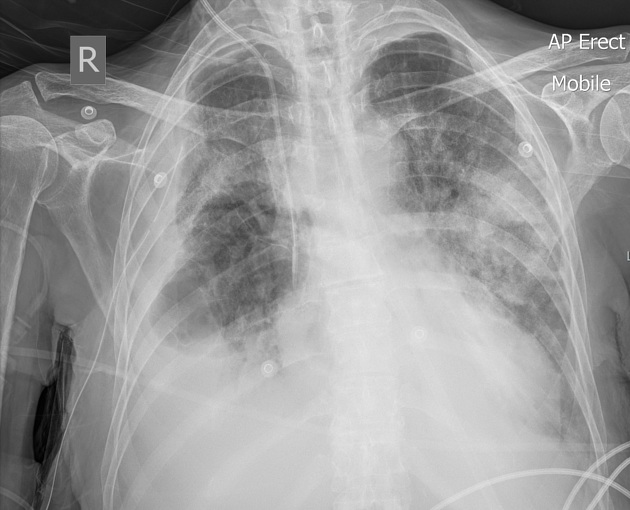
Plain radiograph
Sclerotic bone metastases typically present as radiodense bone lesions that are round/nodular with relatively well-defined margins 3. Radiographs are specific but suffer from low sensitivity 1.
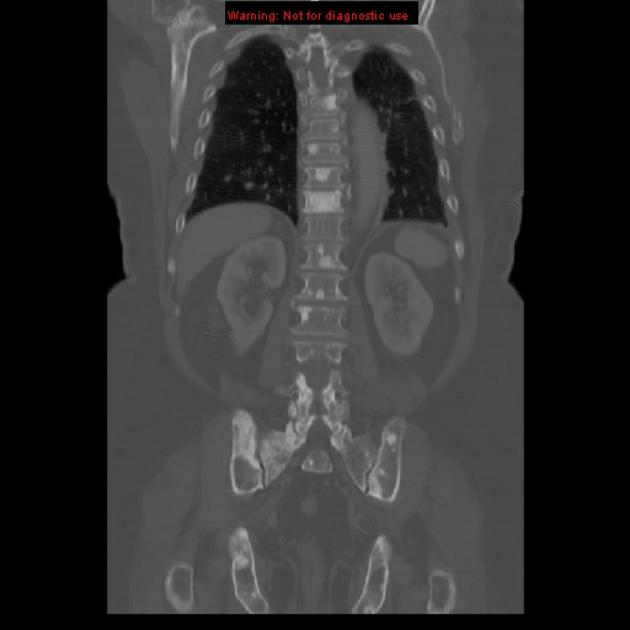
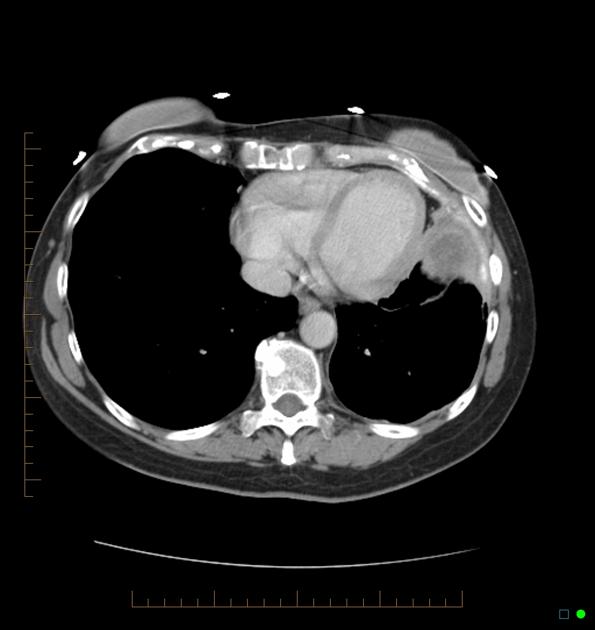
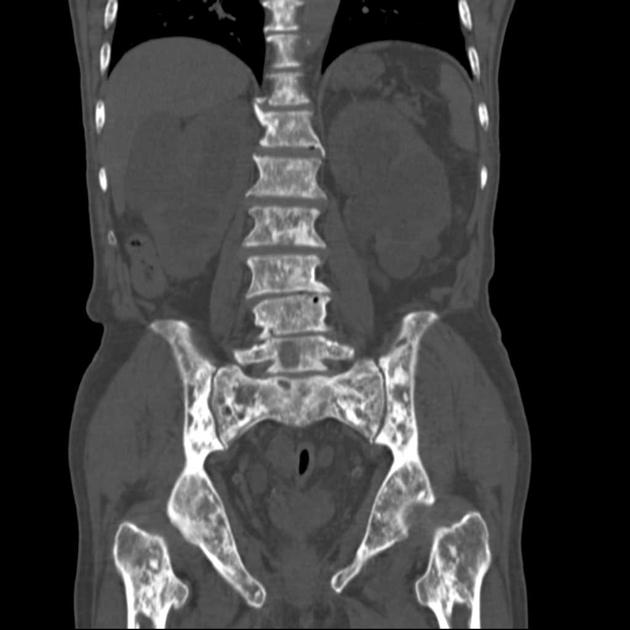
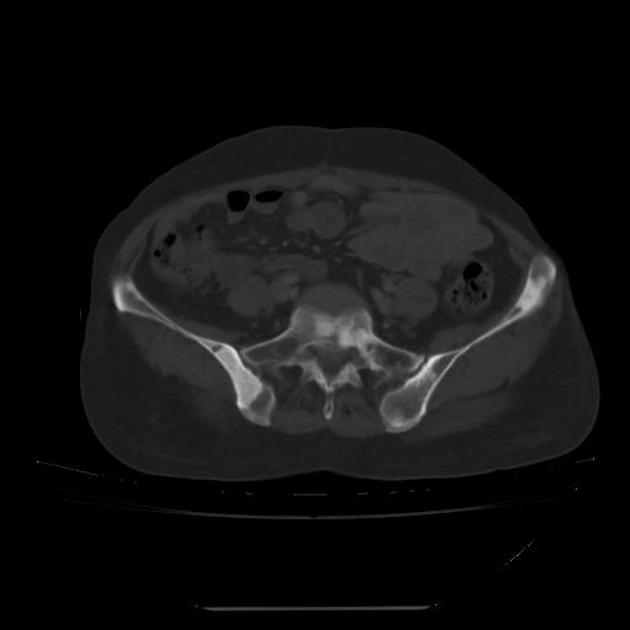
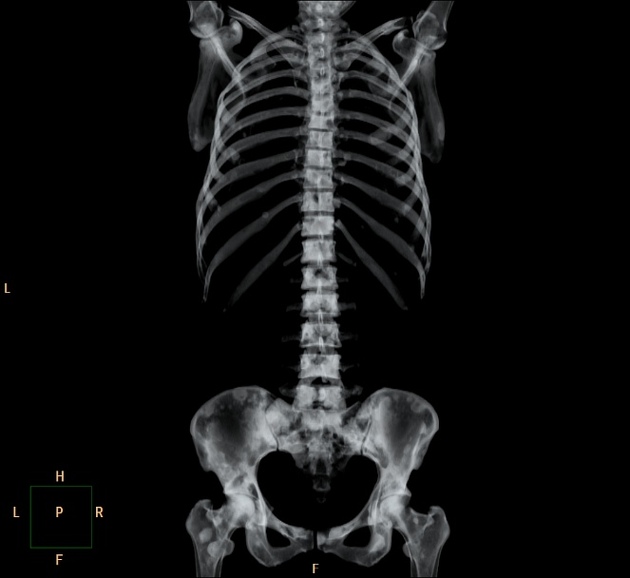
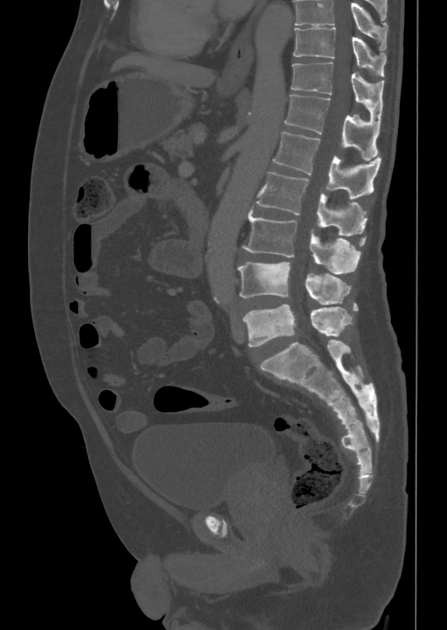
CT
CT can detect osteoblastic metastases with a higher sensitivity than plain radiographs and shines in the assessment of bones characterized by a small bone marrow cavity and a high amount of cortical bone, such as the ribs 2,3.
On CT, sclerotic bone metastases typically present as hyperdense lesions but display a lower density than bone islands 5. A mean CT attenuation threshold of 885 HU and a maximum attenuation threshold of 1060 HU have been found supportive in the differentiation of untreated osteoblastic and bone island in one study 7, but the exclusive use of attenuation values for the assessment of sclerotic bone lesions has been discouraged 8.
MRI
MRI features high sensitivity and specificity for demonstrating bone metastases in general and for assessing the bone marrow 2,3. It can differentiate predominantly osteoblastic from osteolytic bone metastases 9 and easily demonstrate and assess complications such as pathological fractures or spinal cord compression 2,3.
A disadvantage of MRI is that the detection is poor in bones with a small marrow cavity such as the ribs and these bones are better investigated with CT 2,3.
Signal characteristics
T1: low signal intensity
T2: low to isointense 2,9
SWI: low signal intensity on the inverted magnitude and phase images 9
T1 C+ (Gd): variable
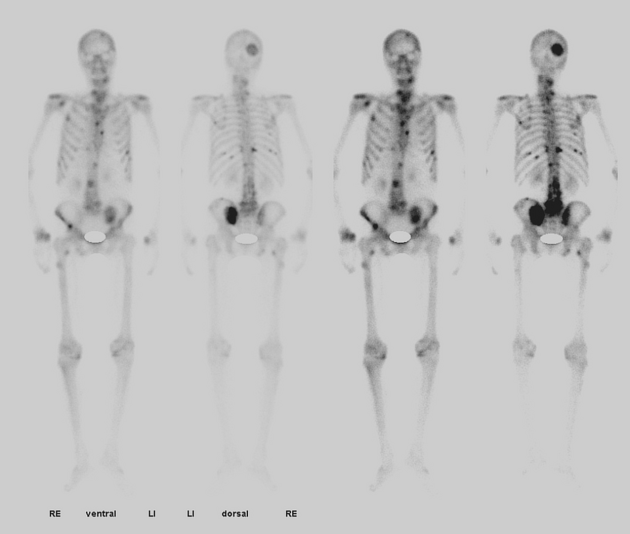
Nuclear medicine
Bone scintigraphy (99mTc MDP) is very sensitive for the detection of osteoblastic providing information on osteoblastic activity but suffers from specificity with a false-positivity rate ranging up to 40% 1.
PET features high sensitivity in the detection of bone metastases especially 18 NaF-PET is suitable for detecting sclerotic metastases since it shows tracer uptake in locations with osteoblastic activity and is more accurate than FDG-PET 3.
Radiology report
The radiological report should include a description of the following 2:
location and size, including the whole extent of disease load
tumor margins and transition zone
-
aggressive features
cortical destruction/breach
pathologic fracture
soft tissue extension
aggressive periosteal reaction
pain attributable to the lesion (if known)
Treatment and prognosis
Treatment of bone metastases, in general, is usually planned by a multidisciplinary team 10. See article: bone metastases
Osteoblastic metastases have a lower fracture risk than lytic or mixed bone metastases 11-13.
Differential diagnosis
post-treatment appearance of any lytic bone metastasis















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.