
Sprengel deformity, or congenital elevation of the scapula, is a complex deformity of the shoulder and is the most common congenital shoulder abnormality. An initial diagnosis can often be made on radiographs, but CT or MRI is often necessary to evaluate the details of the abnormality.
On this page:
Clinical presentation
Sprengel deformity is usually noticed at birth and has both cosmetic and functional implications. The elevated scapula is visually noticeable and there is an associated restriction in the motion of the scapula and glenohumeral joint.
Pathology
Sprengel deformities result from failure of caudal migration of the scapula during early fetal development but the underlying etiology is not known (c. 2012) 12.
Associations
Sprengel deformities usually coexist with other congenital abnormalities, particularly those involving the vertebrae and ribs 12:
omovertebral bar: fibrous, cartilaginous and/or osseous connection between the scapula and cervical spine)
hypoplasia or atrophy of regional muscles
Classification
The Cavendish classification 2,6 is used in both pre-operative and post-operative clinical assessment focussing on cosmetic appearance 9:
grade 0: shoudlers at the same level; no deformity of the superior scapular (rarely used modification to the original classification 9)
grade I: very mild deformity is observed; when covered with clothes the deformity is almost invisible
grade II: the deformity is still mild; the superomedial portion of the high scapula is convex, forming a bump
grade III: moderate deformity with 2-5 cm of visible elevation of the affected shoulder
grade IV: severe deformity with >5 cm elevation of the affected shoulder, accompanied by neck webbing
The Rigault radiographic classification 3,7 is the most commonly used imaging-based system although is yet to be validated (c.2021) as part of clinical assessment 9:
grade I: superomedial angle lower than T2 but above T4 transverse process
grade II: superomedial angle located between C5 and T2 transverse process
grade III: superomedial angle above C5 transverse process
Radiographic features
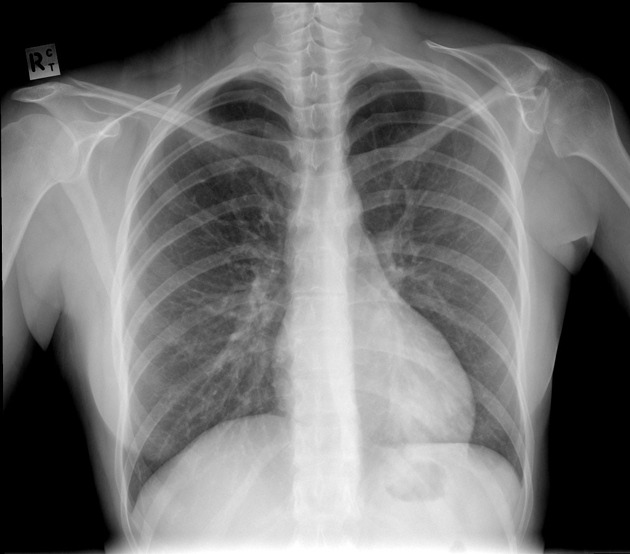
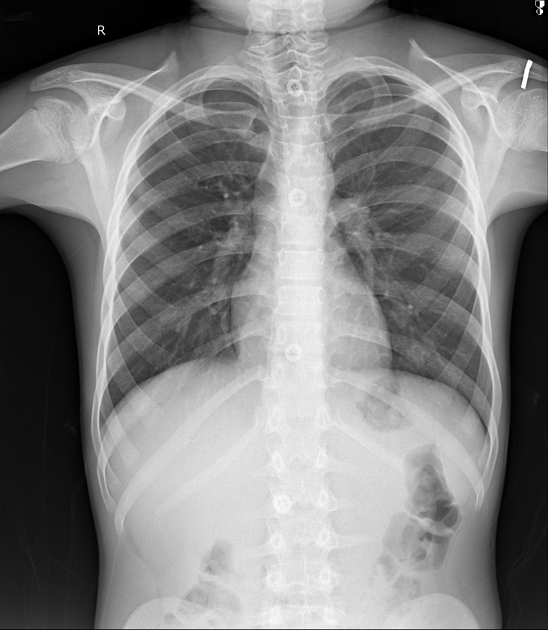
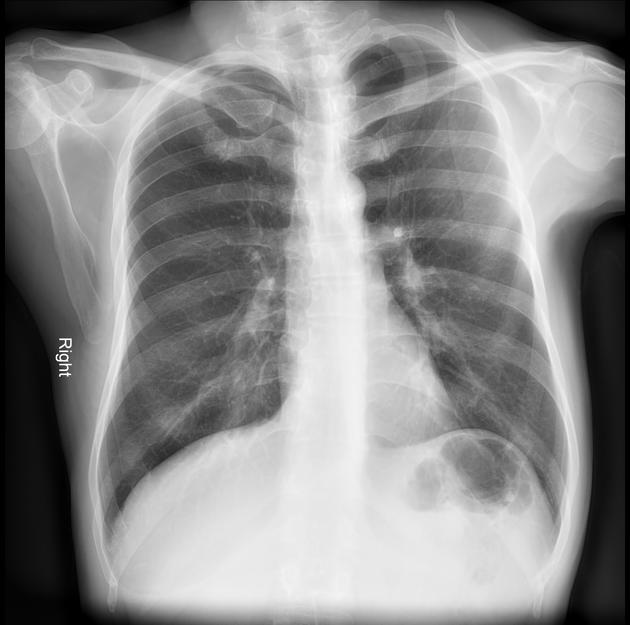
Plain radiograph
The affected scapula is elevated and rotated, with the inferior angle directed laterally.
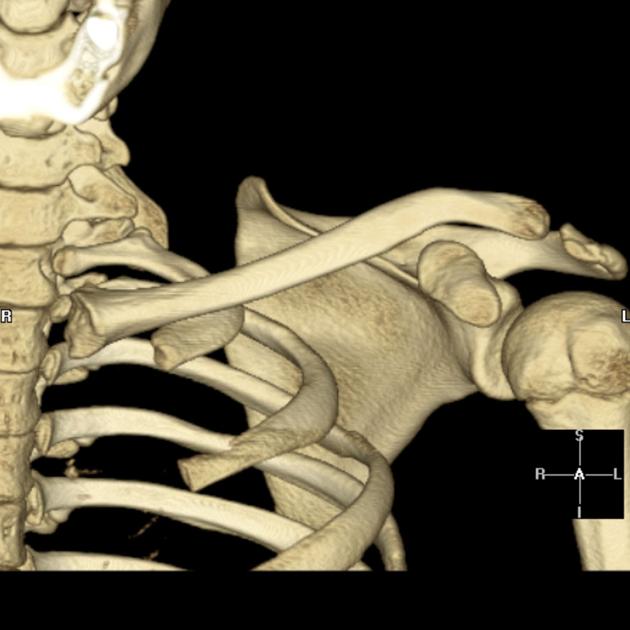
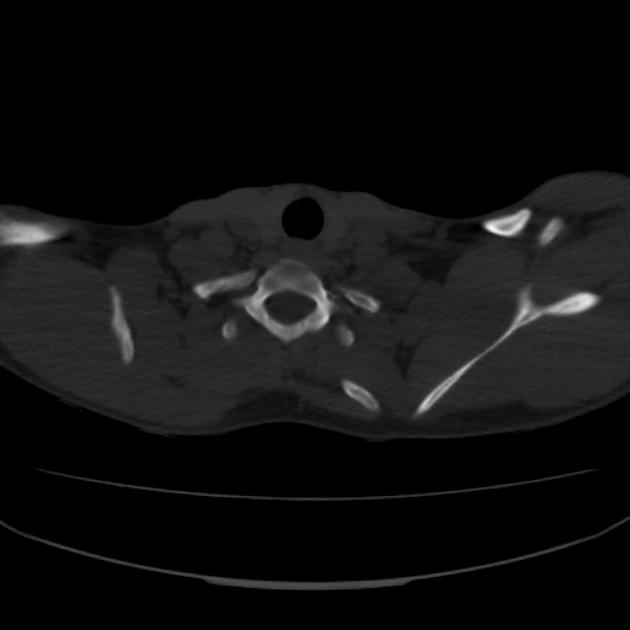
CT
CT with 3D reconstruction is being used to evaluate omovertebral connection and scapula dysplasia and malpositioning. It can be used in preoperative planning.
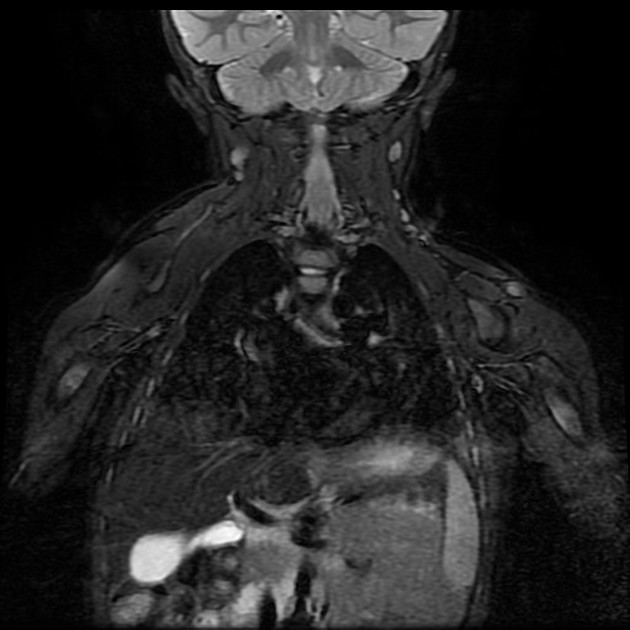
MRI
There may be a role in MRI to assess omovertebral connection.
Treatment and prognosis
Surgery is performed to improve cosmetic and functional disability. It is generally considered for patients between 3 and 8 years of age who have moderate to severe disability or a significant cosmetic abnormality (Cavendish grade 3-4) 1.9. Patients <8 years of age have a 55% rate of restoration of the scapular height (Cavendish grade 0-1), compared to 35% >8 years 9.
Two of the most used surgical methods are the “Woodward” procedure and the “modified-Green” procedure with good functional and cosmetic outcome.
History and etymology
This deformity has the name of Otto Gerhard Karl Sprengel (1852-1915) 8, a German surgeon who described four cases in 189110 although it was first described by another German surgeon, Michael Eulemberg, in 1863 9.
Differential diagnosis
Possible differential diagnosis on presentation:
paralysis (particularly of the long thoracic nerve)
malunited scapular fracture











 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.