
Xanthogranulomatous cholecystitis (XGC) is an uncommon inflammatory disease of the gallbladder that may be difficult to differentiate from malignancy, both on imaging and pathologically. It is characterized by the presence of multiple intramural nodules.
On this page:
Epidemiology
Xanthogranulomatous cholecystitis is seen predominantly in female patients aged 60-80 years old.
Associations
- a relationship with gallbladder carcinoma is uncertain 6,7
Clinical presentation
Patients typically present with symptoms and signs similar to cholecystitis including right upper quadrant pain, vomiting, obstructive jaundice, cholangitis, with a positive Murphy sign and a palpable mass. Leukocytosis is generally present 9.
Pathology
The macroscopic appearance is of a poorly defined, nodular yellow mass that infiltrates the wall of the gallbladder. There is gallbladder wall thickening, and the process may infiltrate directly into the adjacent soft tissues, liver, duodenum, or colon 1.
Histologically, it consists of a mixture of ceroid (wax-like) xanthogranuloma with foamy histiocytes, multinucleated foreign body giant cells, lymphocytes, and fibroblasts containing areas of necrosis.
It is postulated that xanthogranulomatous cholecystitis results from rupture of occluded Rokitansky-Aschoff sinuses, with subsequent intramural extravasation of inspissated bile and mucin 3. This further attracts histiocytes to phagocytize insoluble cholesterol.
The spectrum of pathological findings includes 4,5:
- thickened gallbladder wall: ~90% diffuse and ~10% focal
- infiltration of pericholecystic fat: in 45% focal, in 54% diffuse
- hepatic extension: ~45 %
- biliary obstruction: ~36%
- lymphadenopathy: ~36 %
Radiographic features
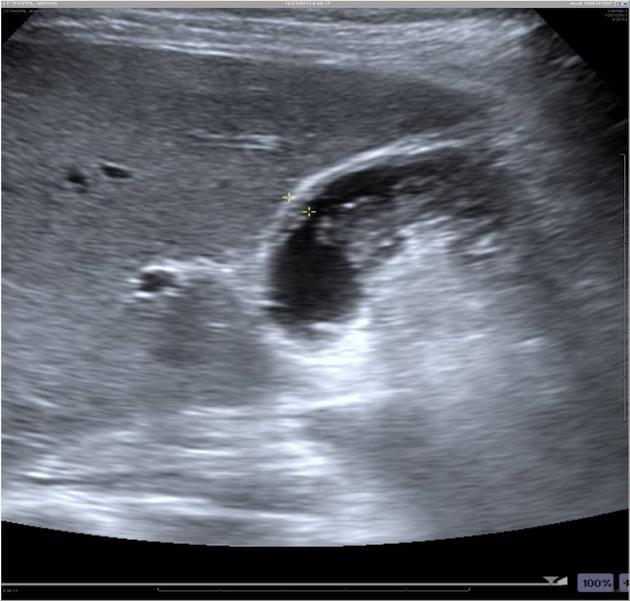
Ultrasound
- gallbladder wall thickening may be diffuse or focal
- intramural hypoechoic nodules or bands
- if the inflammatory process has infiltrated the adjacent liver, there may be loss of the intervening fat plane, with focal hypoechogenicity of hepatic parenchyma
- gallstones often present
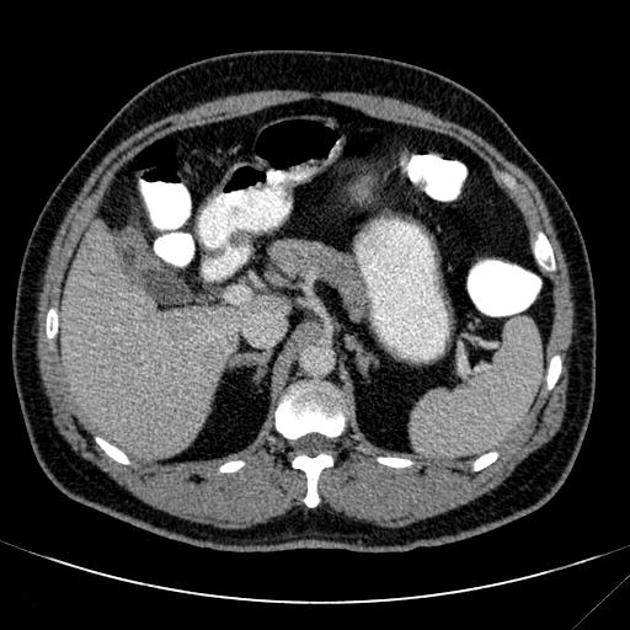
CT
- 5-20 mm small intramural hypoattenuating nodules
- poor/heterogeneous contrast enhancement
- features of local infiltration, or other complications, such as perforation, abscess formation or formation of fistulous tracts 1
Treatment and prognosis
Because of its imaging similarity to gallbladder carcinoma, cholecystectomy is often performed. Fine needle aspiration has been performed to differentiate the two entities.
Differential diagnosis
-
gallbladder carcinoma may be indistinguishable
- the presence of hypoattenuating nodules within the thickened gallbladder wall favors xanthogranulomatous cholecystitis
- acute cholecystitis
- adenomyomatosis
- actinomycosis of the gallbladder 9





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.