
Emphysematous cystitis refers to a gas-forming infection of the bladder wall.
On this page:
Epidemiology
The condition is rare and usually confined to certain patient subgroups. Median age affected is 66 years. More common in women, 2:1 F:M 9.
Risk factors
Risk factors include:
-
considered the commonest predisposing factor 6
may be present in ~50% of cases 2
immunocompromised state
transplant recipients
prolonged catheterization 9
Clinical presentation
Symptoms and signs are similar to those of non-emphysematous cystitis, and maybe very non-specific, e.g. fever, abdominal ache and diarrhea. More specific urinary symptoms, such as dysuria and hematuria may be present. A history of pneumaturia may be seen but is not common.
Most often the diagnosis is made incidentally during an imaging examination.
Complications
Potential complications include:
ureteric and renal parenchymal extension
bladder rupture with sepsis and peritonitis
Pathology
Emphysematous cystitis may be caused by bacterial or fungal infection. The most common causative organism is E. coli, with other organisms including Enterobacter aerogenes, Klebsiella pneumonia, Proteus mirabilis, Staphylococcus aureus, streptococci, Clostridium perfringens and Candida albicans.
The constituent gases responsible are mainly carbon dioxide, nitrogen, hydrogen and methane 9.
Radiographic features
Plain radiograph
Conventional radiography characteristically shows curvilinear or mottled areas of increased radiolucency in the region of the urinary bladder, separate from more posterior rectal gas. Intraluminal gas will be seen as a gas-fluid level that changes with patient position, and, when adjacent to the non-dependent mucosal surface, may have a cobblestone or “beaded necklace” appearance. This is thought to reflect the irregular thickening produced by submucosal blebs as seen at direct cystoscopy.
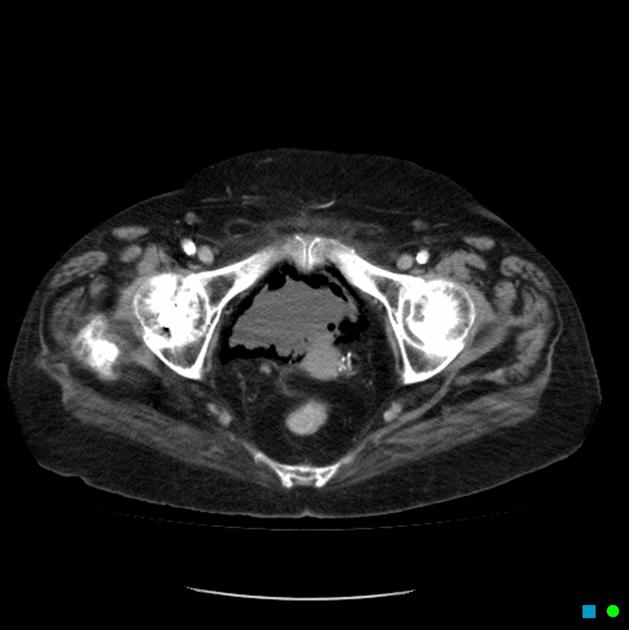
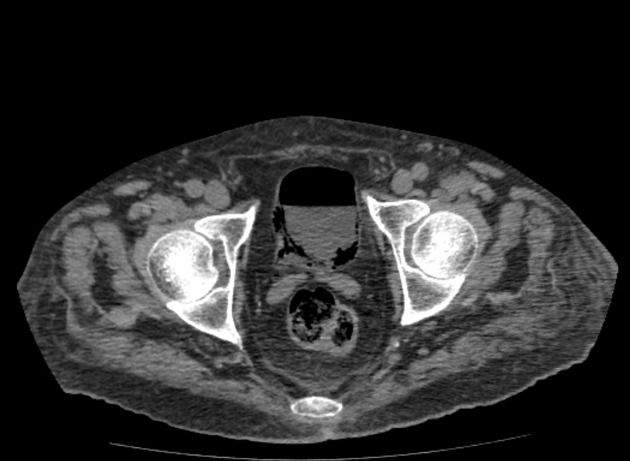
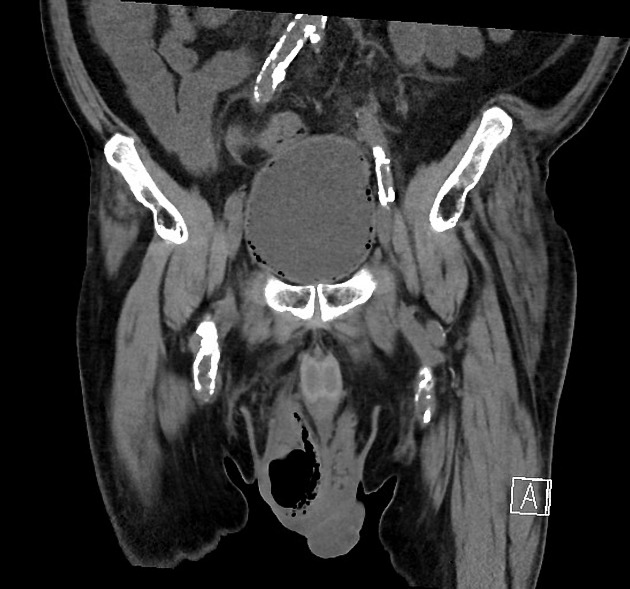
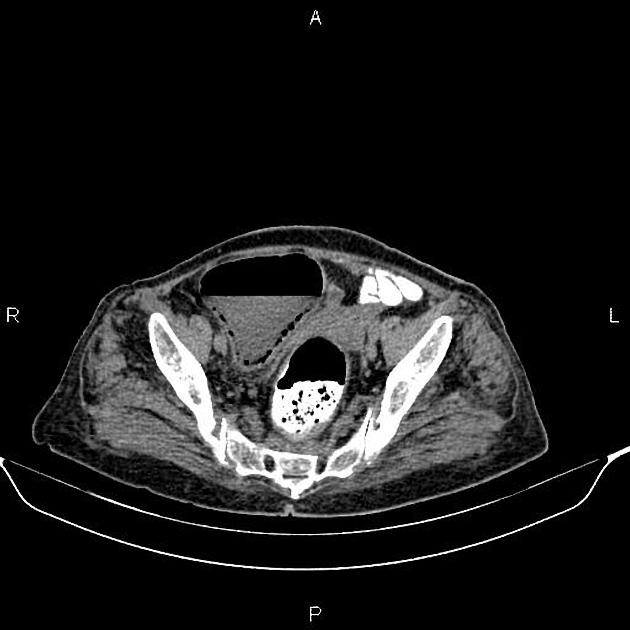
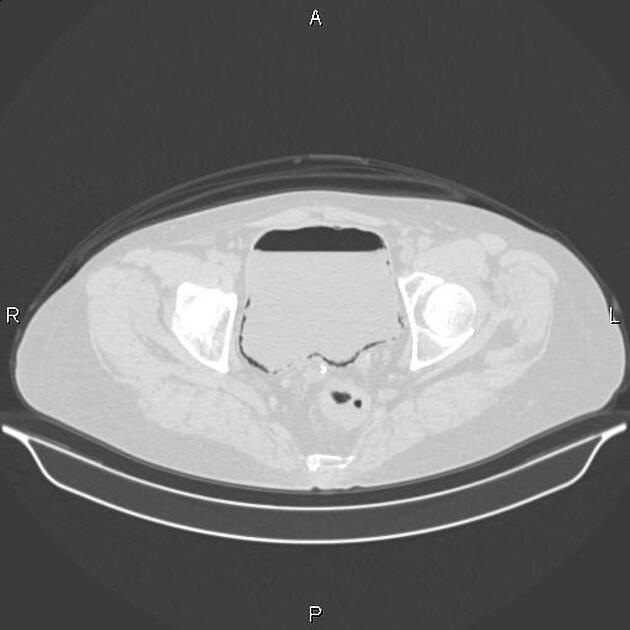
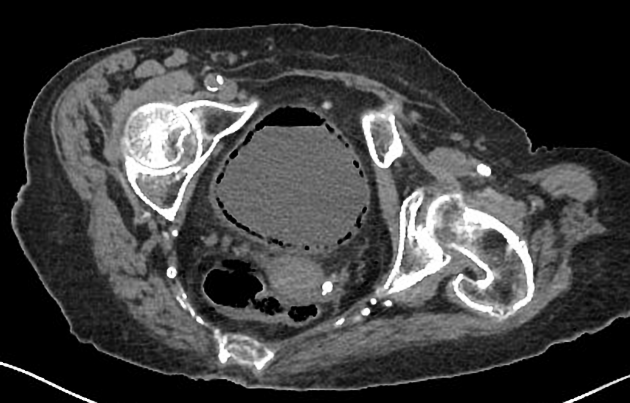
CT
CT is a highly sensitive examination that allows early detection of intraluminal or intramural gas. CT is also useful in evaluating other causes of intraluminal gas such as enteric fistula formation from adjacent bowel carcinoma or inflammatory disease.
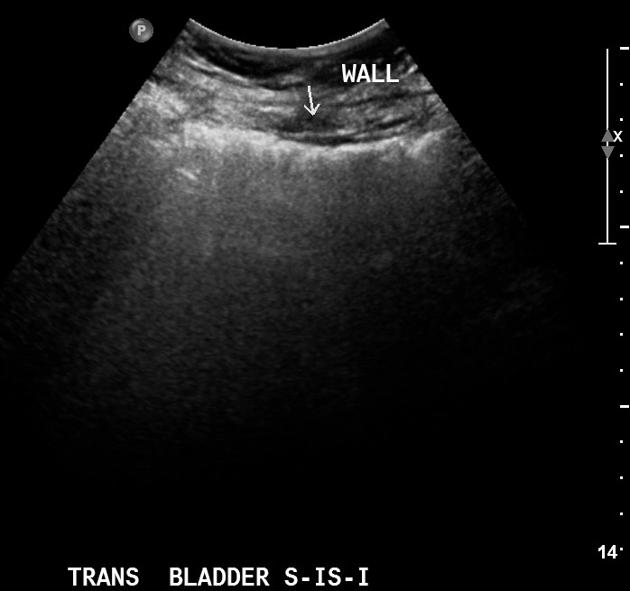
Ultrasound
Can demonstrate echogenic gas within the bladder wall with dirty shadowing artifact. Ultrasound will also commonly demonstrate diffuse bladder wall thickening and increased echogenicity.
Treatment and prognosis
Treatment involves urinary catheterization, antibiotic therapy and control of underlying diabetes.
Differential diagnosis
Gas within the bladder wall is virtually always due to emphysematous cystitis. Intraluminal gas within the bladder has a more broad differential. Be careful not to confuse intraluminal gas with fat density; the latter may be due to chyluria and can be identified using careful windowing.











 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}