
Renal oncocytomas are relatively benign renal tumors. This lesion's main clinical importance is the difficulty in distinguishing it from renal cell carcinoma in the preoperative setting. This is because epidemiology, presentation, imaging and even histology can be very similar.
On this page:
Epidemiology
Renal oncocytomas account for approximately 5% of resected primary adult epithelial renal neoplasms. They typically present in the 6th to 7th decades with a peak incidence at 55 years of age. There is 2:1 male predilection 1,2. Unfortunately, these demographics are similar to renal cell carcinoma.
Associations
Clinical presentation
Up to three-quarters of patients with a renal oncocytoma are asymptomatic. In cases where the mass is large, a flank or abdominal mass may be the presenting complaint. Occasionally hypertension, hematuria or pain may be the presenting complaint 2.
Pathology
Macroscopic appearance
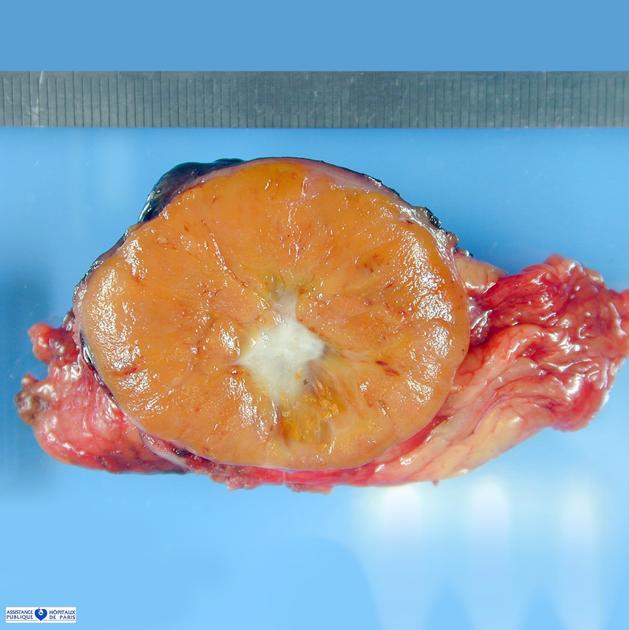
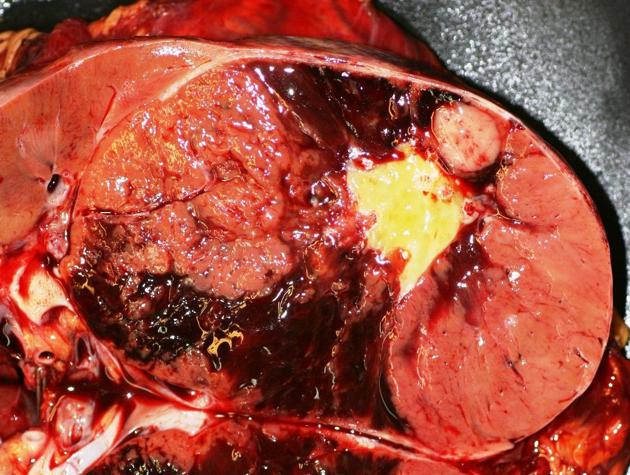
Macroscopically oncocytomas are well-circumscribed, unencapsulated tan in color, similar to the renal cortex, or darker brown (mahogany brown) 13. A rim of compressed normal renal parenchyma is sometimes seen, forming a pseudocapsule 2,3. A central radiating scar is identifiable in approximately in 33% of cases and is related to size of tumor 13. Macroscopic hemorrhage is seen in a minority of patients (~20%) 2.
Microscopic appearance
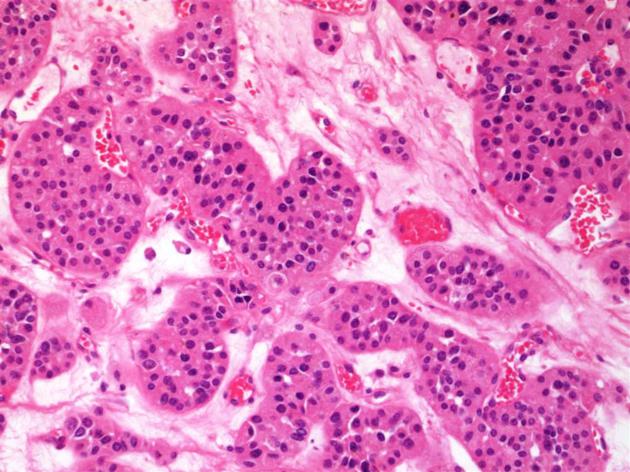
Oncocytomas are believed to originate from intercalated tubular cells of the collecting tubules and are composed of acini, tubules or microcysts placed within a hyalinized stroma. Tumor composed of round to polygonal large, swollen cells with eosinophilic and granular cytoplasm ,round nuclei and central nucleolus . A biopsy is usually unhelpful in distinguishing an oncocytoma from a renal cell carcinoma, as the latter may also have oncocytic elements 5. Mitotic activity is rarely seen but necrosis and atypical mitosis are usually absent 3. Oncocytoma is a benign neoplasm so nuclear grading system the ISUP/ WHO criteria should not be used 13.
Radiographic features
Unfortunately, the imaging appearance of oncocytomas is difficult to distinguish from renal cell carcinoma, and as such, they are usually resected 5. They appear as sharply demarcated lesions of variable size, but often large at presentation. A potentially helpful sign is the presence of a sharp central stellate scar, which although characteristic of oncocytomas, is only seen in a third of cases 7. Additionally, renal cell carcinomas may also demonstrate a central scar 5.
The only reliable feature is evidence of metastasis or aggressive infiltration into adjacent structures, in which case the diagnosis of renal cell carcinoma can be safely made.
It is important to carefully evaluate both kidneys, as up to 13% of patients have multiple oncocytomas (renal oncocytosis), and up to 32% have concurrent renal cell carcinomas 2.
Intravenous pyelogram
Oncocytomas appear as sharply demarcated, often large, exophytic masses with enhancement during the nephrographic phase.
Ultrasound
Ultrasound demonstrates a well-circumscribed mass with echogenicity similar to the rest of the kidney. Occasionally a central scar may be visible 5.
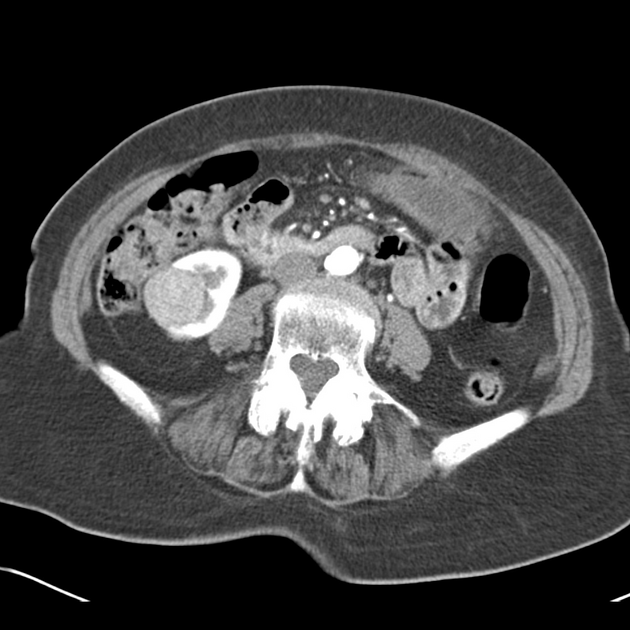
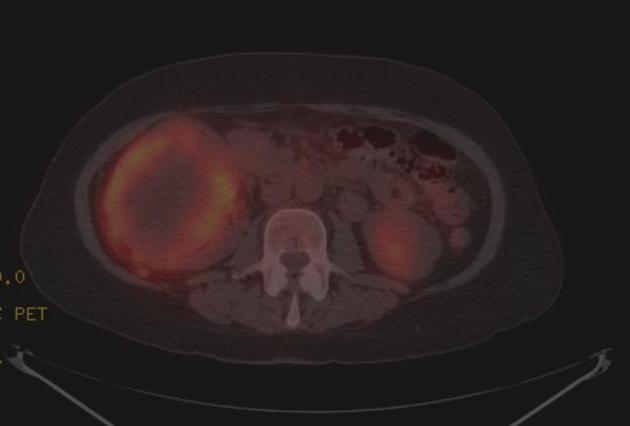
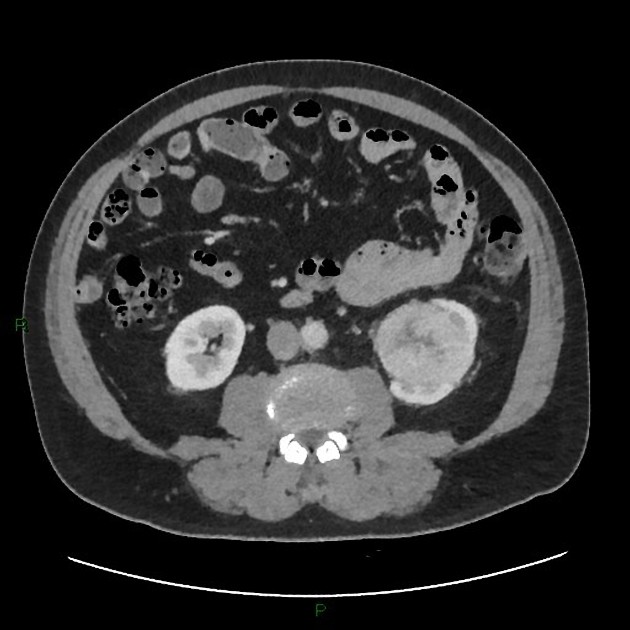
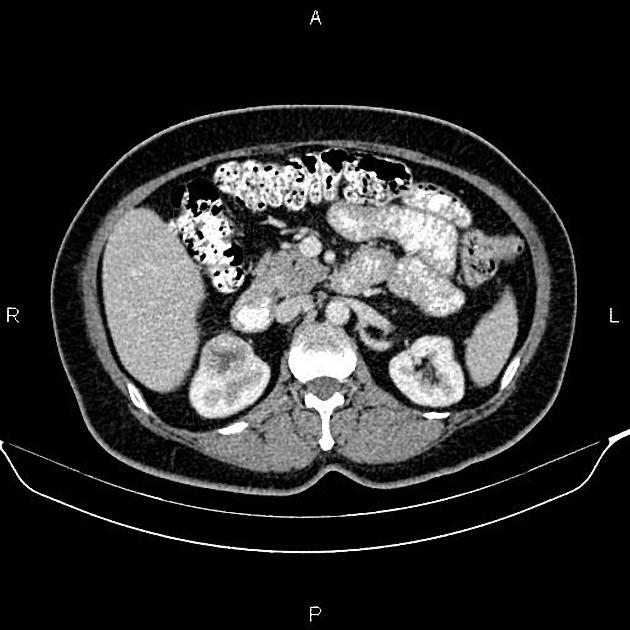
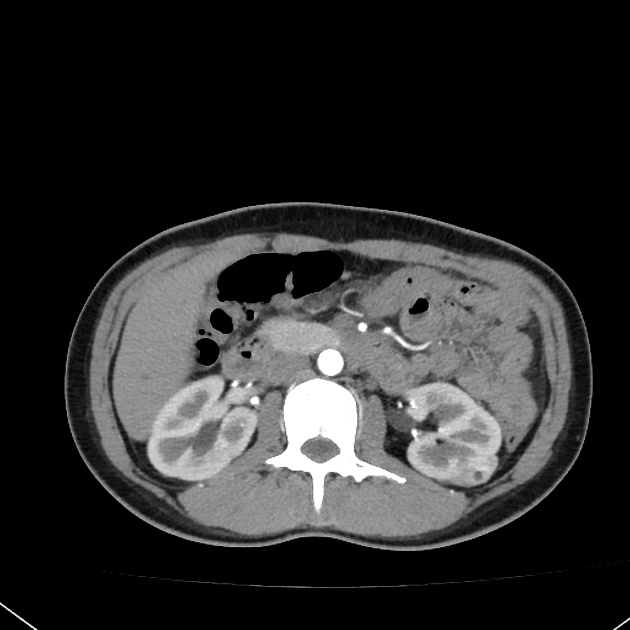
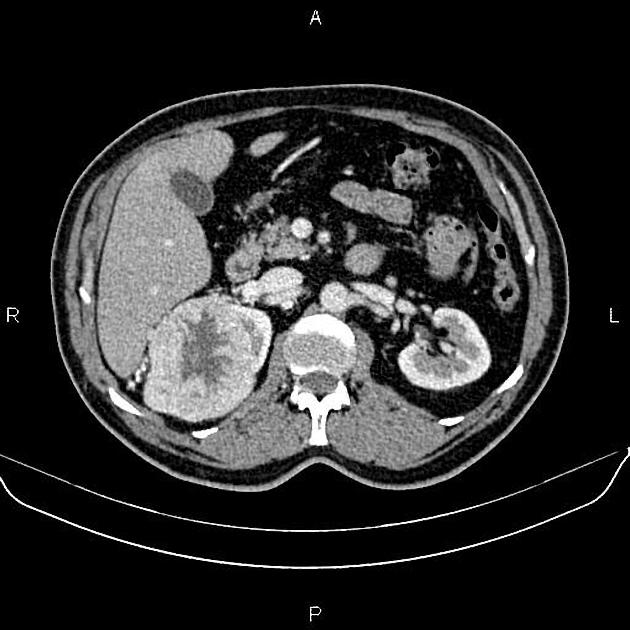
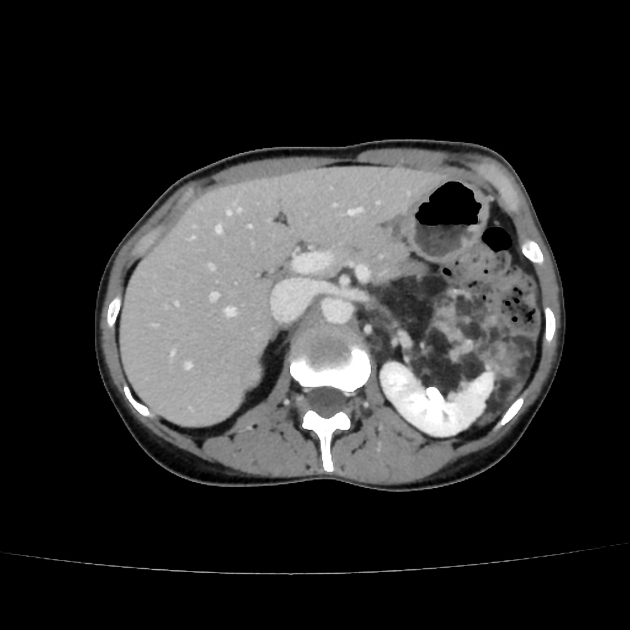
CT
Tend to be large well-demarcated tumors at presentation.
Non-contrast
<3 cm: homogenous attenuation 8
>3 cm: heterogeneous attenuation
perinephric fat stranding may be present due to edema
calcification may be present
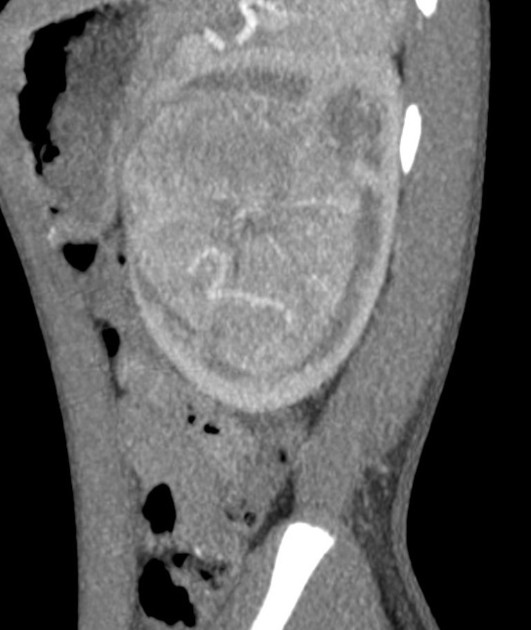
Post-contrast
small tumors may enhance homogeneously, but usually enhancement is heterogeneous and the mass is larger
central stellate non-enhancing scar is seen in approximately a third of cases 7
renal vein thrombosis may be present, but tumor thrombus is absent
-
segmental enhancement inversion 9
two distinct regions of differing segmental enhancement in the corticomedullary phase, with the enhancement pattern inverting during the nephrogenic phase
more common in tumors <3 cm
MRI
Typical signal characteristics include:
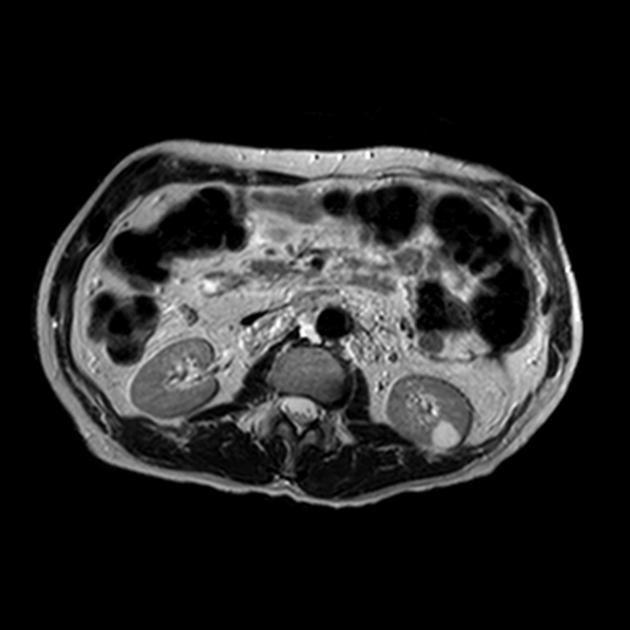
T1: hypointense compared to renal cortex 10
-
T2
hyperintense compared to renal cortex
may demonstrate hypointense central stellate scar
T1 C+ (Gd): usually demonstrates homogeneous enhancement
Angiography (DSA)
May demonstrate a spoke wheel pattern, of peripheral circumferential vessels penetrating towards the center of the lesion, which again, although characteristic of oncocytomas, may also be seen in renal cell carcinomas.
During the capillary phase, the tumor demonstrates a homogeneous blush, similar to normal renal parenchyma, lacking the 'bizarre' vascularity typically seen in renal cell carcinoma 3,5,11. A lucent avascular rim may be seen due to the compressed pseudocapsule 3.
Microaneurysms have occasionally been reported 3.
Treatment and prognosis
Although renal oncocytomas are benign lesions and metastases are extremely uncommon 2,12, they cannot be confidently distinguished from renal cell carcinomas preoperatively, and therefore they are surgically resected. If the diagnosis is suspected preoperatively then renal sparing surgery can be performed.
Differential diagnosis
General imaging differential considerations include
-
the imaging appearances of renal cell carcinomas and oncocytomas overlap to such a degree that confident preoperative distinction is often not possible
Practical points
biopsy may be unhelpful in distinguishing an oncocytoma from a renal cell carcinoma, as the latter may also have oncocytic elements
gross invasion of perirenal fat, tumoral extension into the renal vein, and regional lymphadenopathy on imaging would favor renal cell carcinoma instead of oncocytoma







 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.