
Renal artery stenosis (RAS) (plural: stenoses) refers to a narrowing of a renal artery. When the process occurs slowly, it leads to secondary hypertension. Acute renal artery stenosis does not lead to hypersecretion of renin.
Pathology
When the stenosis occurs slowly, collateral vessels form and supply the kidney. The kidney wrongly senses the reduced flow as low blood pressure (via the juxtaglomerular apparatus) and releases a large amount of renin that converts angiotensinogen to angiotensin I. Angiotensin I is then converted to angiotensin II with the help of angiotensin-converting enzyme (ACE) in the lungs. Angiotensin II is responsible for vasoconstriction and release of aldosterone which causes sodium and water retention, thus resulting in secondary hypertension.
Etiology
Renal artery stenosis may be caused by several pathological processes:
atherosclerosis (~75% of cases): involves the proximal renal artery
fibromuscular dysplasia (~20%): involves the distal renal artery, younger population
vasculitides: especially polyarteritis nodosa (PAN) (causes multiple microaneurysms), Takayasu arteritis, radiation
neurofibromatosis type 1: most commonly involves the ostium
compression by diaphragmatic crura 11,12
Occurrence is not uncommon following a renal transplant.
Radiographic features
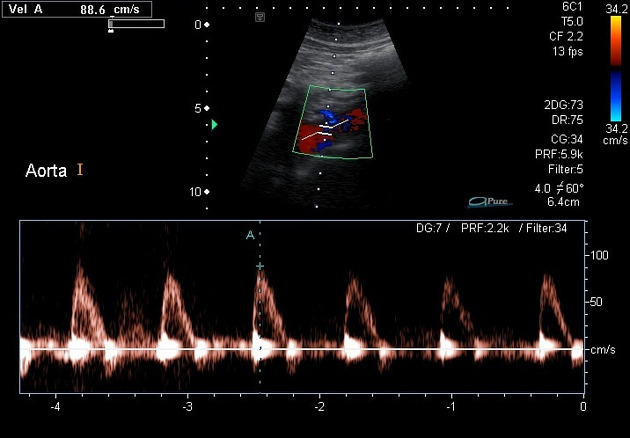
Ultrasound
Ultrasound, although most freely available, cheap and often used first-line, is relatively operator-dependent and may prove time-consuming.
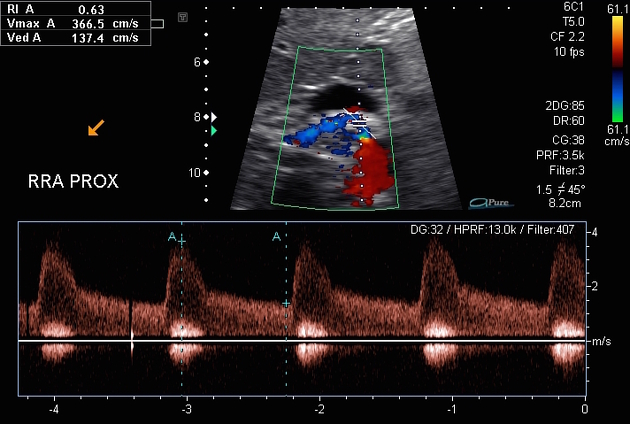
increased peak systolic velocity (PSV): some advocate 180 cm/s 4
increased renal-interlobar ratio (RIR), i.e. PSVrenal artery (intrastenotic)/PSVinterlobar (distal): some advocate values greater than 5 3
-
increased renal-aortic ratio (RAR), i.e. PSVrenal/PSVaorta: usually taken as >3.5, although some advocate >3 4 or even >2 3
lower cut off values increase sensitivity but decrease specificity
turbulent flow in a post-stenotic area
pulsus parvus et tardus waveform (slow-rising) due to stenosis
decreased (interlobar) renal arterial resistive index (RI): <0.55 in severe stenosis 10
resistive index difference between kidneys >5% 9
acceleration index (AI): lower than 3 m/s2
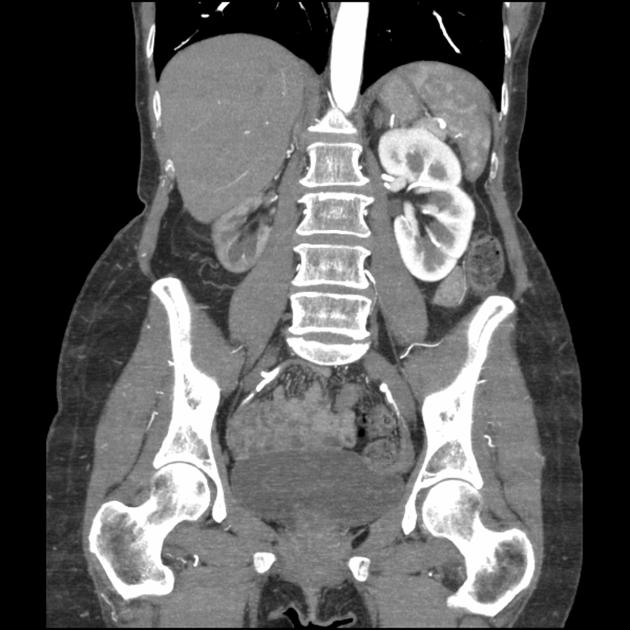
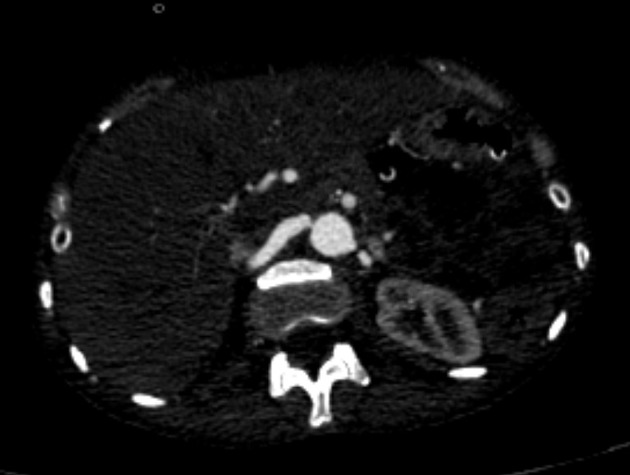
CT
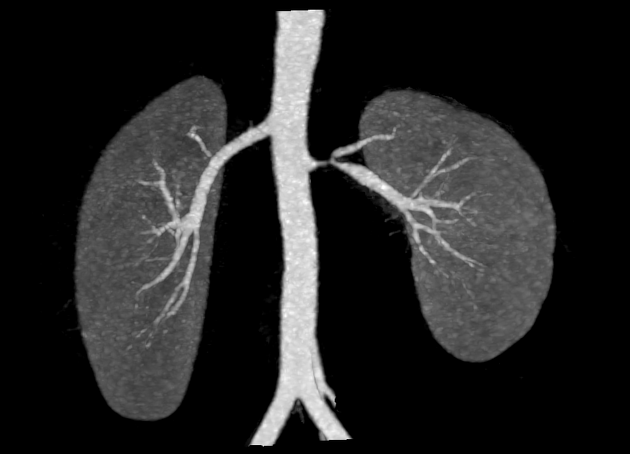
The three-dimensional reconstruction of the renal vascular tree provides a reliable method of visualizing the entire vascular tree. Images are acquired with thin collimation and bolus tracking on the abdominal aorta. Sensitivity and specificity of 90-99% have been reported 7. Both the raw data and 3D reconstructions should be viewed. Additionally, supernumerary arteries may be identified.
MRI
Different imaging methods can be used for renal MRA:
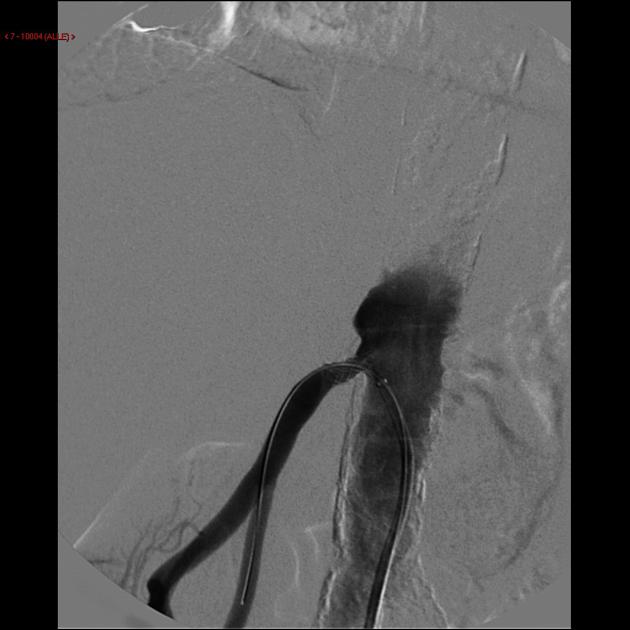
time of flight (TOF): whereby the high velocity of the blood jet at the level of stenosis appears as a loss of signal (black)
phase contrast technique
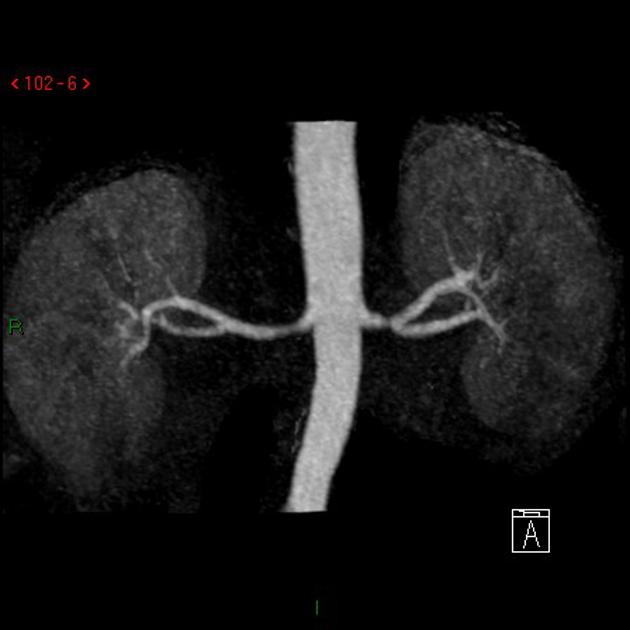
contrast-enhanced MRA: gadolinium is used as a contrast agent
Three-dimensional reconstruction technique offers sensitivity and specificity values around 90-100% 7. In some cases, renal impairment does not permit the use of contrast, in which case TOF imaging is beneficial.
Reported sensitivity and specificity for MR angiography is at around >95%; >90% for detection of stenoses of 50% or greater in diameter. MR angiography may overestimate moderate stenosis and detection/evaluation of multiple and branch arteries can at times be problematic.
Nuclear medicine
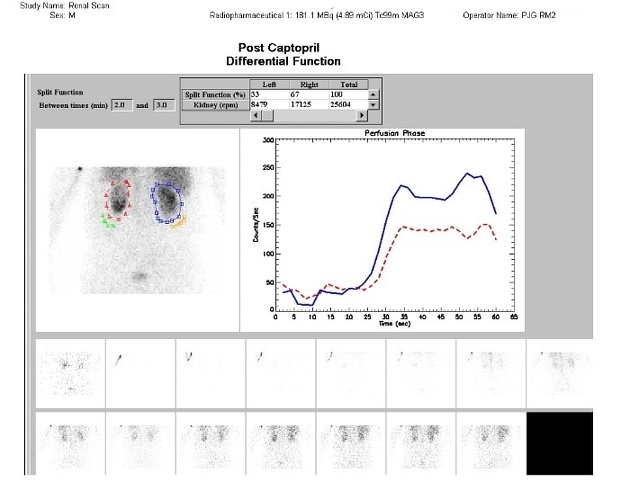
ACE inhibitor scintigraphy
the affected kidney with renovascular hypertension shows impaired function due to ACE inhibition; based on this principle scintigraphy has been very much useful for the diagnosis of renal artery stenosis
performed by IV administration of enalapril maleate after 15 minutes
sequential images and scintigraphic curves are plotted for the renal cortex and pelvis; renal uptake is measured every 1-2 minute interval after administering the IV injection
typical isotopes used are Tc-99m MAG3, Tc-99m DTPA or I-123 ortho-iodohippurate 6
interpreted as either low, intermediate or high probability






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.