
Bladder calculi, commonly referred to as bladder stones, are urinary stones that are found primarily in the urinary bladder and comprise only 5% of all urinary tract stones. They can be divided into primary, secondary, and migratory stones:
primary: bladder stones form in the absence of other urinary tract abnormality, typically seen in children in endemic areas
secondary: stones form in an abnormal bladder or from concretions on foreign material (e.g. urinary catheters)
migratory: usually renal calculi which have migrated down into the bladder; uncommon
On this page:
Epidemiology
Primary bladder stones are now uncommon in developed countries, and the incidence is continuously declining. However, the incidence is still quite high in developing countries, especially in North Africa, the Middle East, and Southeast Asia endemic areas. This is due to poor hydration, recurrent diarrhea, and a diet deficient in animal protein.
Family history is found in up to a third of idiopathic cases 2.
Secondary bladder stones are due to urinary stasis, including from:
foreign body, e.g.: indwelling Foley catheter, retained fragment from a removed Foley catheter, surgical sutures (nonabsorbable)
bladder augmentation (not with gastric tissue)
Migratory stones are either a renal stone or a sloughed renal papilla that serves as a nidus for formation of a bladder stone. This type of stone is uncommon, as virtually any stone that can pass though the ureter, can also pass on through the urethra. A stone will stay stuck in the urinary bladder due to bladder outlet obstruction or bladder dysfunction (similarly to secondary stones), and may be laminated by material other than that of the original stone.
Clinical presentation
Bladder calculi may present with pain, infection, or hematuria. In some cases, they may be asymptomatic.
Radiographic features
Plain radiograph
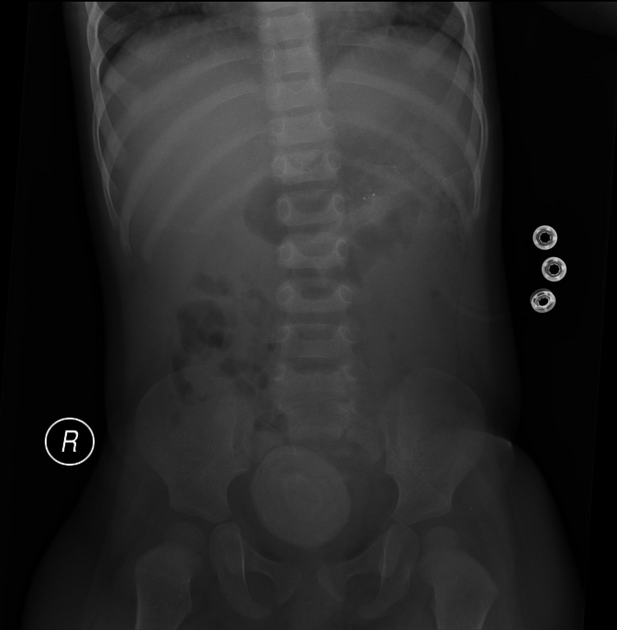
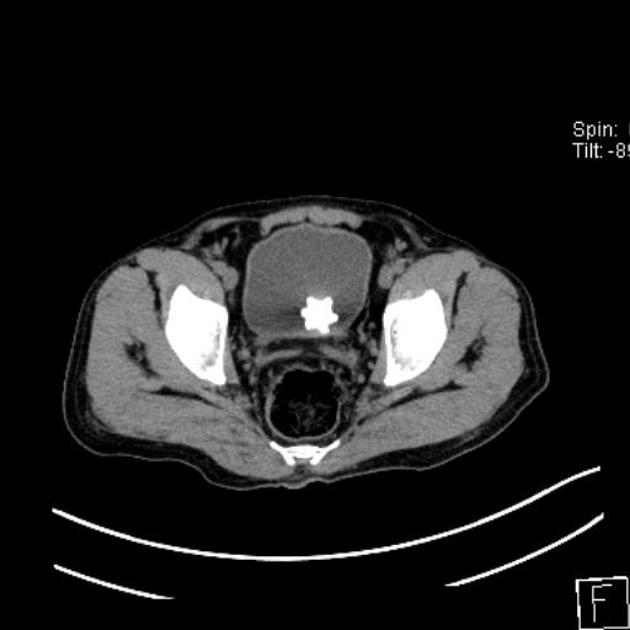
Usually densely radiopaque, calculi may be single or multiple and are often large. Frequently lamination is observed internally, like the skin of an onion.
Ultrasound
Sonographically they are mobile, echogenic, and shadow posteriorly. They may be associated with bladder wall thickening due to inflammation.
Treatment and prognosis
The earliest method of operative removal of bladder calculus was performed via the perineal route with the patient in a supine position and the legs elevated, hence the term lithotomy position.
Differential diagnosis
occasionally a calculus which appears to be in the bladder is actually in the distalmost part of the ureterovesical junction: rescanning the patient in the prone position can help to distinguish these from true bladder calculi
for a tiny calculus abutting the anterior margin of the bladder at supine CT, consider a calcification at the insertion of a urachal remnant into the urinary bladder 4
for other pelvic calcifications on plain film just outside the outline of the bladder, consider entities such as vascular calcification, most commonly phleboliths


























 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.