
Tubo-ovarian abscesses are one of the late complications of pelvic inflammatory disease.
On this page:
Epidemiology
Risk factors
Risk factors for tubo-ovarian abscesses include 15:
previous pelvic inflammatory disease 16
multiple sexual partners
history of uterine surgery (e.g. post hysterectomy) 16
Clinical presentation
Patients typically present with a combination of fever, elevated inflammatory markers, lower abdominopelvic pain, and vaginal discharge. Fever and leukocytosis may sometimes be absent.
Pathology
Abscesses are often polymicrobial with a preponderance of anaerobic organisms 9.
Uncommon causes include actinomycosis, tuberculosis, and xanthogranulomatous inflammation 17.
Radiographic features
The clinical context is extremely important in radiological interpretation. Patients will experience tenderness with endovaginal scanning. Some differentiate between:
tubo-ovarian "abscess": ovary and tube cannot be separately distinguished within the inflammatory mass
tubo-ovarian "complex": if the tube and ovary are separately discernible structures within the inflammatory mass
Plain radiograph
Features are non-specific and may include:
soft tissue density mass
loss of normal pelvic fat planes
an adynamic ileus may be present
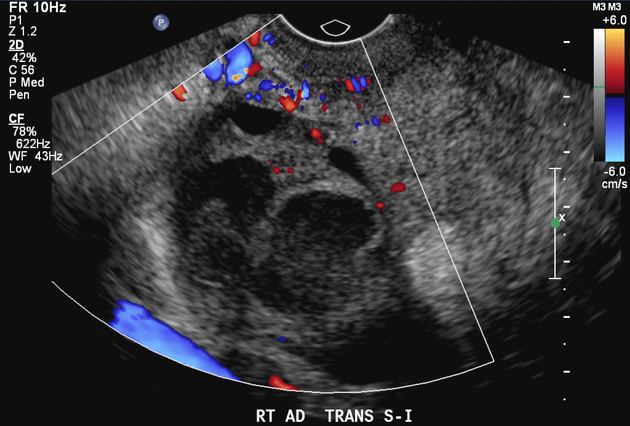
Ultrasound
Transabdominal and endovaginal ultrasound are the preferred initial imaging investigations. Findings may include:
-
multilocular complex retro uterine/adnexal mass
debris, septations, and irregular thick walls
commonly bilateral
echogenic debris within the pelvis
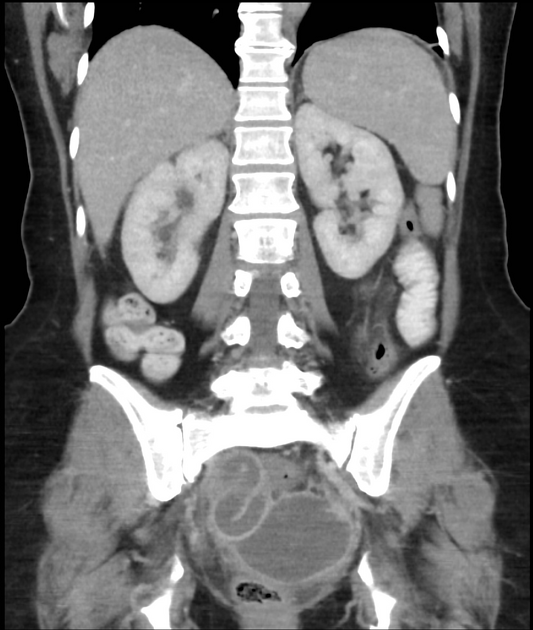
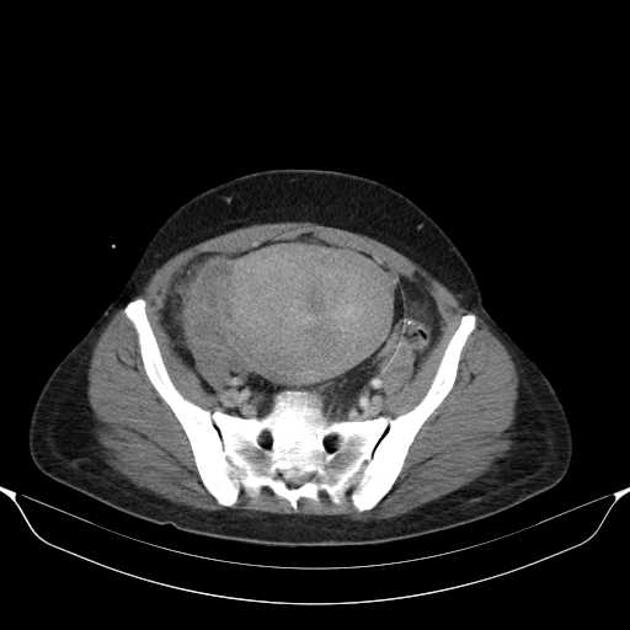
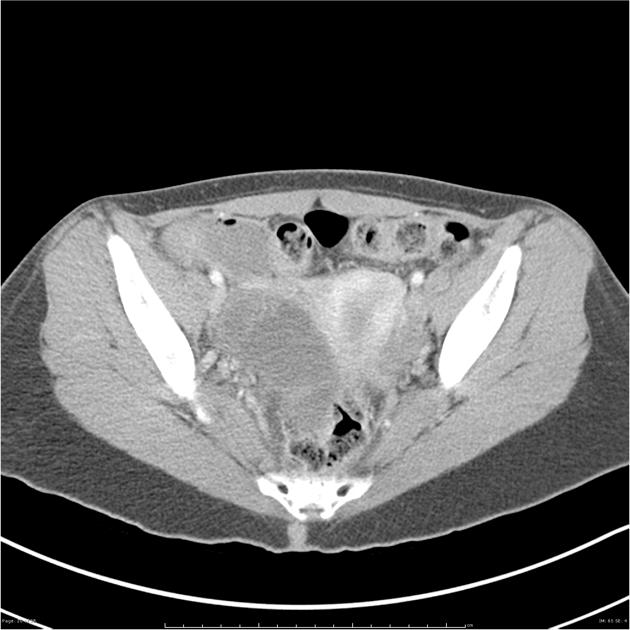
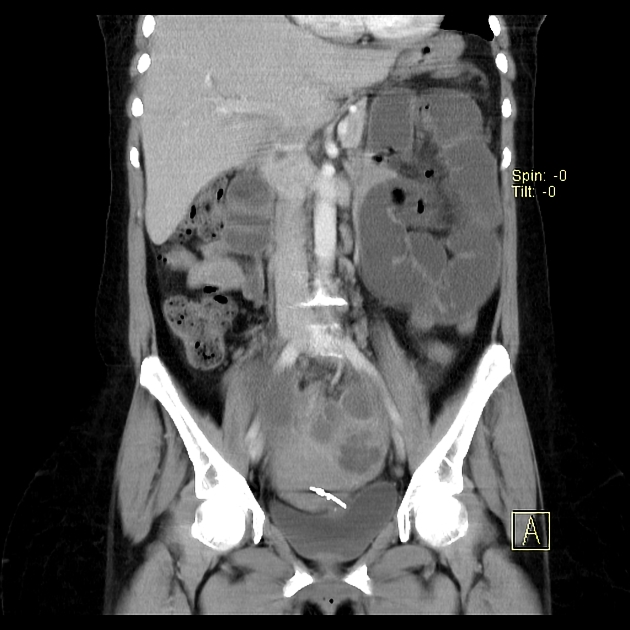
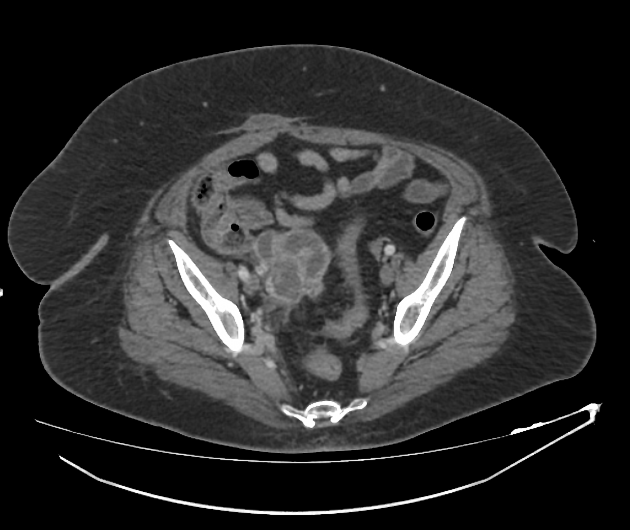
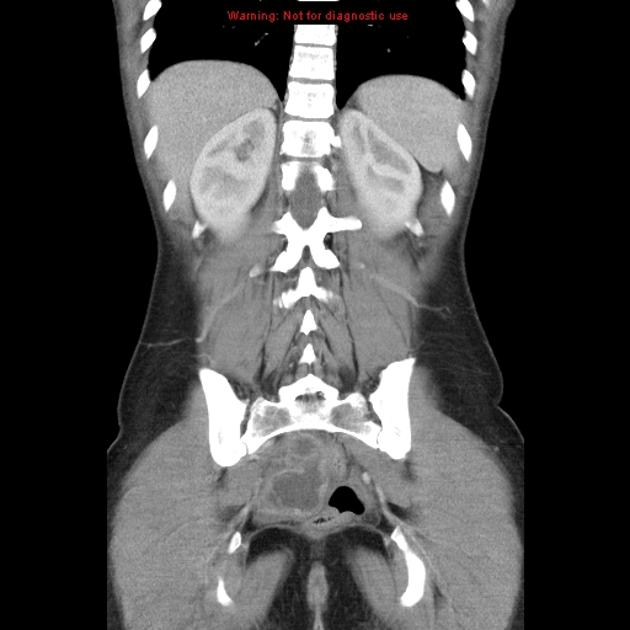
CT
Can be a helpful adjunct to ultrasound, especially in determining the extent of disease 3,18:
high attenuation fluid pelvic masses which may contain fluid-fluid levels or gas
usually shows a thick enhancing abscess wall
a tubular multilocular configuration is more conclusive of a pyosalpinx
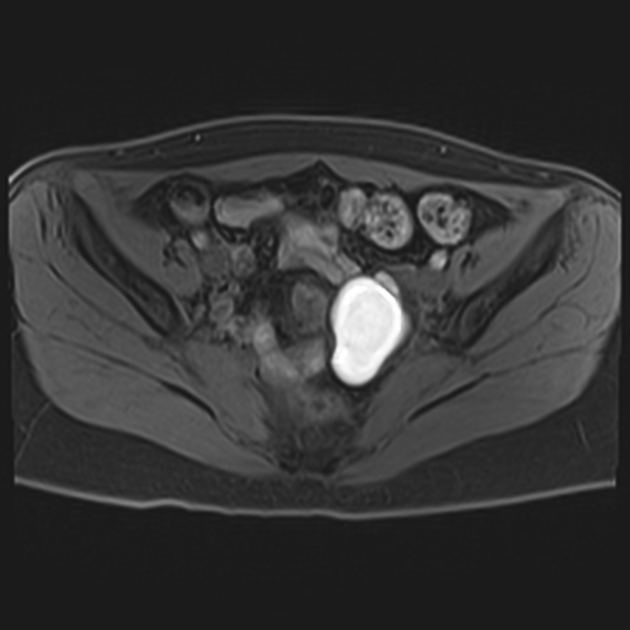
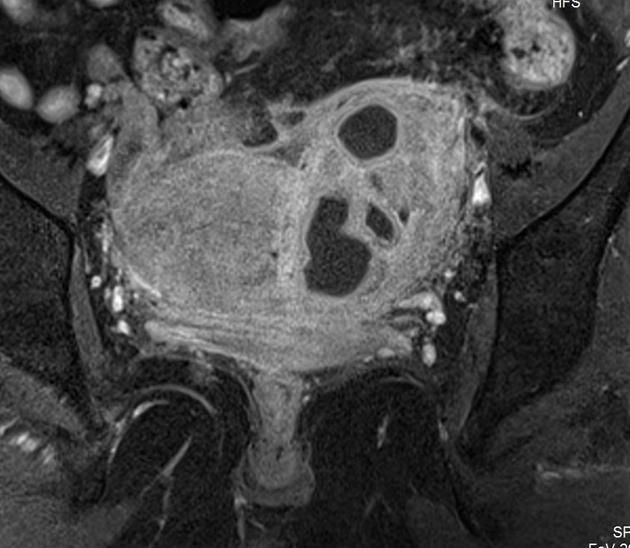
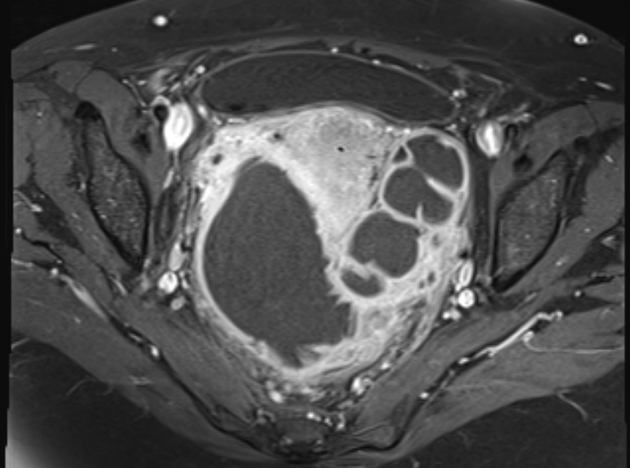
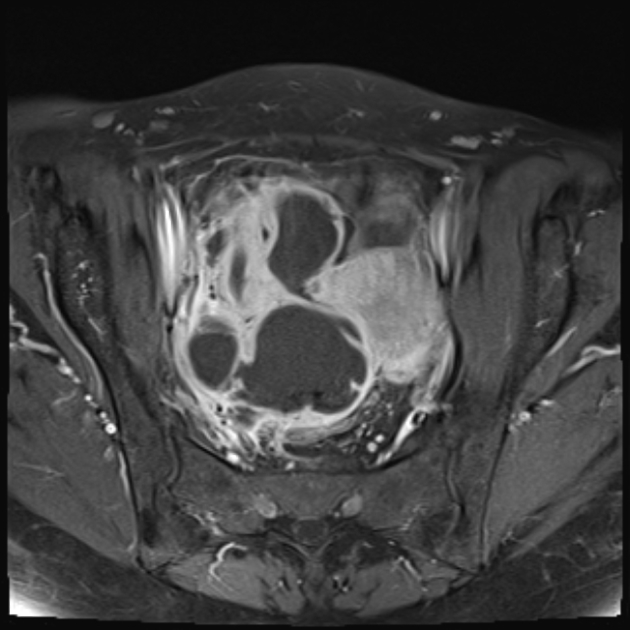
MRI
Can be useful especially when sonography is inconclusive or if the gas content is difficult to be differentiated from bowel gas 5.
Typically seen as thick-walled fluid-filled pelvic mass(es) 12
T1: abscess contents typically hypointense
T2: abscess contents typically heterogeneous signal or hyper-intense
Treatment and prognosis
Initial treatment can be with antibiotic therapy. Radiologically guided drainage or surgery may be required in patients resistant to antibiotic treatment. Drainage may be performed from an endovaginal, transgluteal, or transabdominal approach, dependent on patient and operator preference 4.
Recognized complications include:
abscess rupture
rarely, perihepatitis (Fitz-Hugh-Curtis syndrome) 14
Differential diagnosis
Clinical features of infection is key to aid diagnosis as a number of other pathologies can give similar appearances 1:
complex diverticular abscess
complex appendiceal abscess
pelvic endometriosis
pelvic hematoma
Uncommon causes of tubo-ovarian abscesses such as actinomyces and tuberculosis have many overlapping features with ovarian malignancy, including:
relatively vague presentation
solid/cystic ovarian masses
peritoneal and/or serosal thickening and enhancement
There may be clues that favor uncommon causes of tubo-ovarian abscesses over malignancy:
long-standing intrauterine contraceptive device as a risk factor for actinomyces
smoother peritoneal enhancement more typical of peritonitis rather than carcinomatosis
In these cases, biopsy or fluid sampling is often most appropriate to guide therapy and avoid unnecessary surgical intervention 17.













 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.