
Uterine lipoleiomyomas result from degeneration of smooth muscle cells in an ordinary leiomyoma and represent a rare benign tumor of the uterus 1.
On this page:
Epidemiology
Lipoleiomyomas have a reported incidence of 0.03-0.20% and are typically found in postmenopausal patients with typical uterine leiomyomas 2.
Clinical presentation
Although most patients are asymptomatic, they can present with symptoms similar to leiomyomas of the same size and location. Symptoms include, but are not limited to, abdominal/pelvic pain, palpable mass, and menstrual abnormalities.
Pathology
Many considered uterine lipoleiomyoma as a distinct variety of leiomyoma. Histologically, it is composed of variable amounts of adipocytes and smooth muscle cells, separated by thin fibrous tissue. The exact etiology is not well known but is thought to represent fatty metaplasia of the smooth muscle cells of a leiomyoma.
They are most commonly located intramurally within the body of the uterus, although can originate anywhere along the uterus (including the cervix) and also may be subserosal 3. Lesions can vary in size from a few millimeters to a few centimeters.
Radiographic features
Leiomyolipomas slightly vary in appearance depending on their composition. They generally appear as benign uterine masses resembling fibroids, except that there is a component of bulk fat. Advanced imaging of these lesions allows for differentiation from cystic ovarian neoplasms, which may require surgical therapy 3.
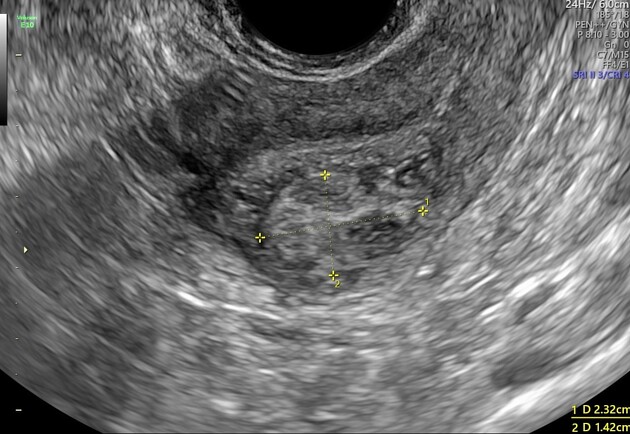
Ultrasound
-
hyperechoic with a partially hypoechoic rim
the rim likely represents a layer of myometrium surrounding the fatty central component 3
posterior acoustic attenuation
often poor vascularity on color Doppler examination
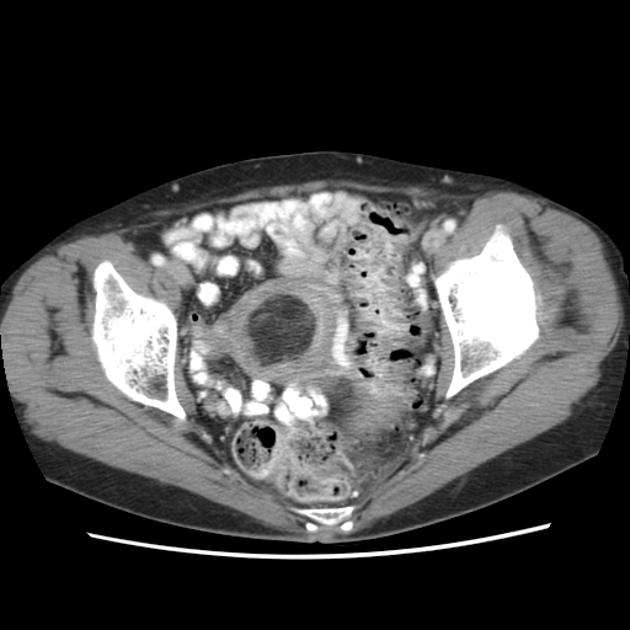
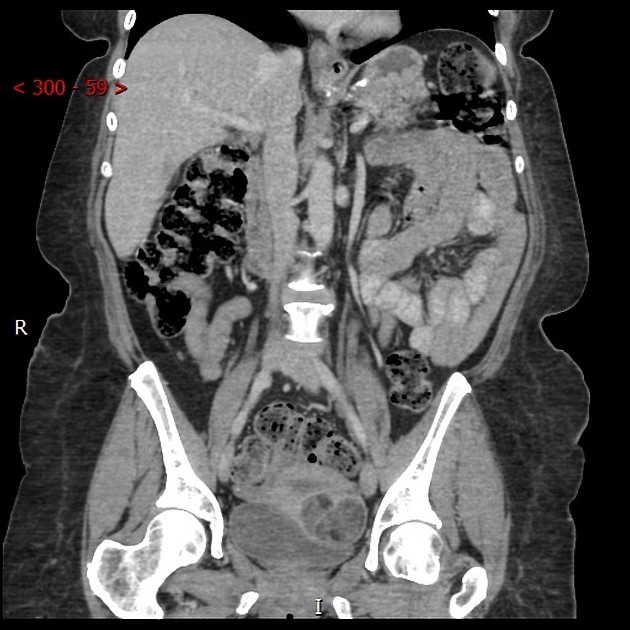
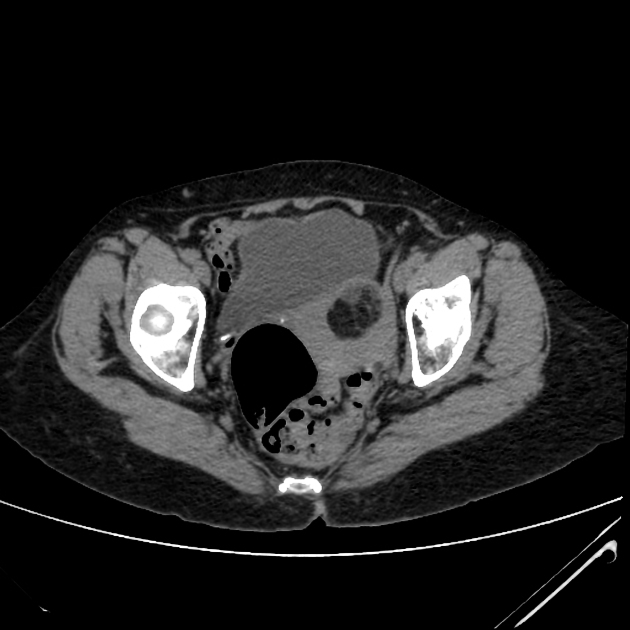
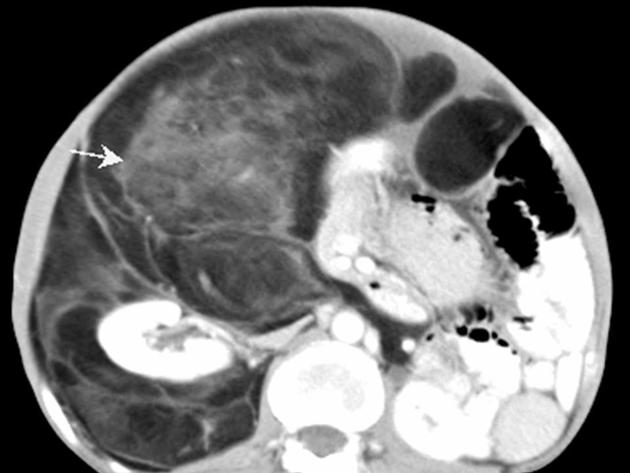
CT
predominantly fat-containing mass arising from uterus, typically measuring between -40 to -100 HU
well-marginated
often contains areas of soft tissue density
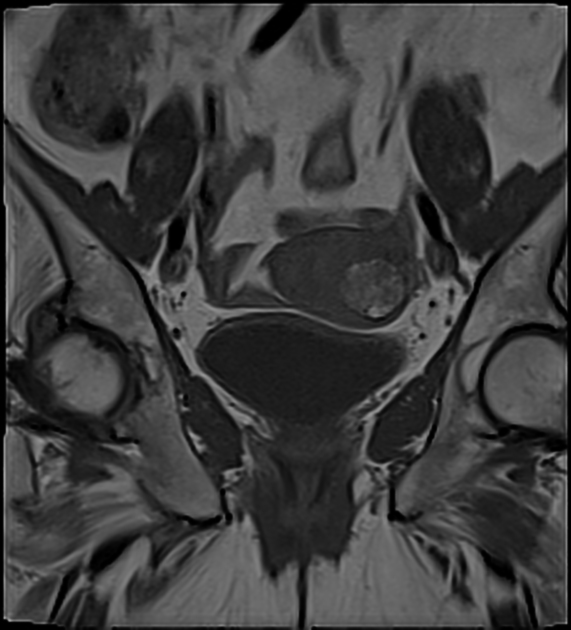
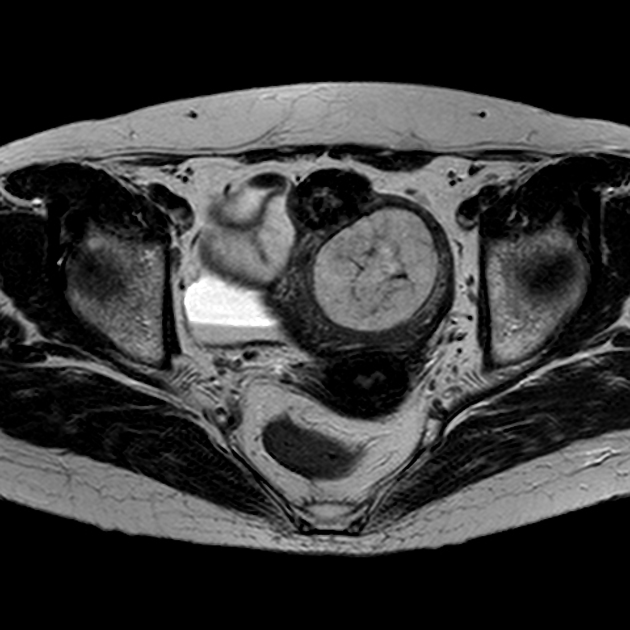
MRI
Secondary to the predominant fatty component in the lesion, hyperintensity is seen on T1 weighted sequences and chemical shift artifacts are noted. Additionally, fat suppression techniques can be useful in verifying the diagnosis - most of the lesion shows fat suppression 3. Signal characteristics are, therefore:
T1: hyperintensity
T1 FS: hypointensity (saturates out)
T2: hyperintensity
T2 FS or STIR: hypointensity (saturates out)
Treatment and prognosis
Lipoleiomyomas when small and asymptomatic usually do not require treatment and are clinically similar to leiomyomas. Treatment is similar to leiomyomas and is dependent on the clinical symptoms and the size/location of the lesion. Uterine artery embolization or surgical excision can be performed, as indicated 1. In general, they are benign tumors with favorable prognosis.
History and etymology
The first report as a "myolipoma of soft tissue" was thought to have been described in 1991 by Meis and Enzinger 4.
Differential diagnosis
General imaging differential considerations include:
benign cystic ovarian teratoma
malignant degeneration of cystic teratoma
pelvic lipoma
pelvic liposarcoma
-
very rare lipomatous tumors of the uterus:









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.