
Varicocele is the dilatation of the pampiniform plexus of veins, a network of many small veins found in the male spermatic cord. It is the most frequently encountered mass of the spermatic cord.
On this page:
Epidemiology
The estimated incidence is at ~15% of the general male population and ~40% of subfertile and infertile men (the most common cause of correctable male infertility).
Varicocele is rare in children under the age of ten years. However, it may be seen in up to 15–20% of adolescents and young men and as high as 42% in elderly men 7,8.
Clinical presentation
Varicocele can be asymptomatic. If symptomatic, presentations include:
scrotal mass/swelling
scrotal pain
infertility or subfertility
Pathology
The pampiniform veins normally act as heat exchangers, important in the thermoregulation of the testes which is vital for spermatogenesis. Testicular temperature is normally maintained at 35ºC. A varicocele disturbs this balance and causes the testis to heat up to the normal core body temperature (37ºC).
Etiology
A varicocele can be classified as primary or secondary.
Primary varicocele
Most varicoceles are primary and result from incompetent or congenitally absent valves in the testicular vein (internal spermatic vein).
The left testis is affected much more commonly (≈85%) than the right. This may be due to the shorter course of the right testicular vein and its oblique insertion into the inferior vena cava (IVC) which creates less backpressure. In contrast, the left testicular vein has a longer course and inserts into the left renal vein at a right angle. Bilateral varicoceles are not uncommon (≈15%), but an isolated right varicocele is rare and should prompt evaluation for a secondary varicocele.
Secondary varicocele
Secondary varicocele is much less common and results from increased pressure in the testicular vein due to compression (e.g. extrinsic mass such as retroperitoneal lymphadenopathy or renal mass, or renal vein compression in nutcracker syndrome 9), obstruction (e.g. renal vein thrombosis), or splenorenal shunting (portal hypertension).
Variants
Radiographic features
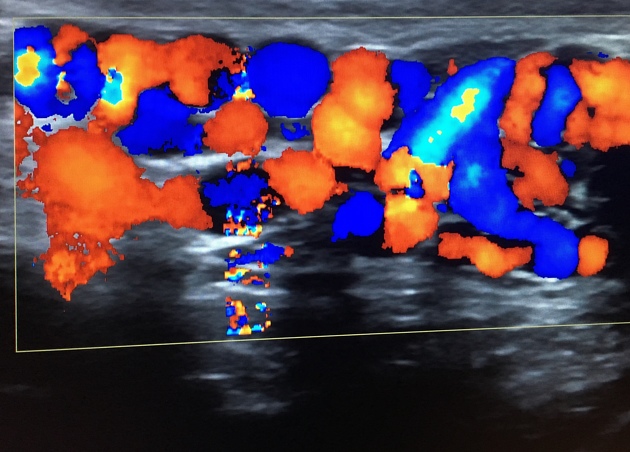
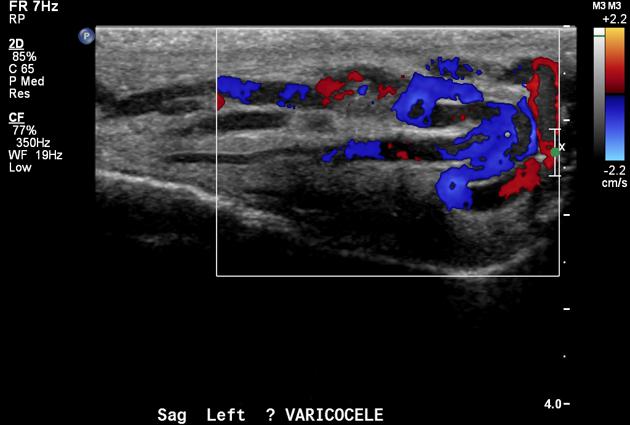
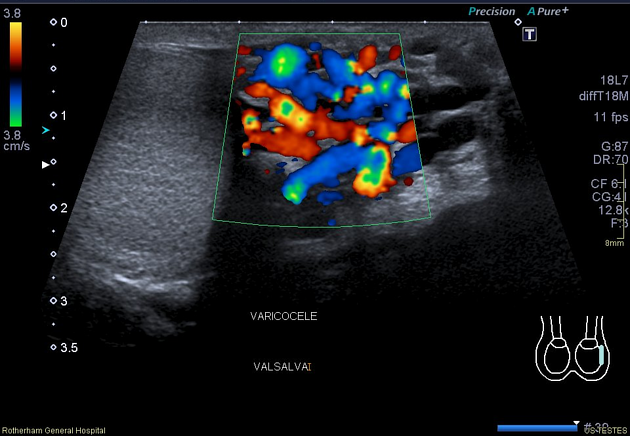
Ultrasound
The diagnostic modality of choice:
dilatation of pampiniform plexus veins >2-3 mm in diameter 3,4
characteristically have a serpentine appearance
there can be flow reversal with the Valsalva maneuver 4
Doppler ultrasound can be used to grade the degree of reflux
CT
may show a dilated cluster of enhancing serpiginous veins
Angiography (DSA)
Venography, only performed during endovascular treatment, may demonstrate:
dilated testicular veins
retrograde flow of contrast towards the scrotum
dilated pampiniform plexus should not be directly imaged as the testes should be kept out of the x-ray beam
MRI
varicocele may be incidentally noted during scrotal MRI
dilated enhancing serpiginous veins
-
signal intensity depends on the velocity of flow
low flow: intermediate T1 and high T2
high flow: signal void
enhancement following gadolinium administration
Treatment and prognosis
This is one of the surgically correctable causes of male infertility. Management options include:
A unilateral right-sided varicocele is an uncommon finding and, if found, should prompt an evaluation of the retroperitoneum to exclude a mass obstructing the downstream testicular vein.









 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.